Miranda L G Hallquist, Juliann M Savatt, Kristy Diloreto, Alicia Johns, Amie Decker, Cameron Hayes, Melissa A Kelly, Henry Lester Kirchner, Natasha T Strande, Adam H Buchanan
{"title":"Increased colorectal and endometrial cancer rates in a genomically ascertained Lynch syndrome cohort.","authors":"Miranda L G Hallquist, Juliann M Savatt, Kristy Diloreto, Alicia Johns, Amie Decker, Cameron Hayes, Melissa A Kelly, Henry Lester Kirchner, Natasha T Strande, Adam H Buchanan","doi":"10.1093/jncics/pkaf061","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lynch syndrome (LS) is a hereditary cancer predisposition that increases risk for colorectal, endometrial, and other cancers. Although population-based genomic screening programs identify individuals with LS, clinical presentation in such genomically ascertained populations is unknown.</p><p><strong>Methods: </strong>MyCode is a healthcare system-based biobank that returns clinically actionable genomic screening results to participants, including pathogenic/likely pathogenic (P/LP) variants in LS genes (MLH1, MSH2, MSH6, PMS2). Adult cases (participants with an LS result) and controls (participants without a cancer predisposition variant matched to cases) reported their personal and family cancer histories. Rates of meeting National Comprehensive Cancer Network (NCCN) genetic testing guidelines and rates of colorectal and endometrial cancers in cases, controls, and their family members were calculated and compared.</p><p><strong>Results: </strong>A total of 175 cases (10 MLH1, 7 MSH2, 83 MSH6, and 75 PMS2) and 169 controls were included. Of case pedigrees, 62/175 (35.4%) met NCCN criteria for LS evaluation. Case pedigrees were more likely (P < .001) to meet criteria than control pedigrees (4/169, 8.35%). Case probands had significantly higher rates of colorectal and endometrial cancer than controls (7.7% vs 2.4%, P = .03 colorectal; 11.5% vs 0%, P < .001 endometrial), as did their relatives (3.1% vs 0.9%, P < .001 colorectal; 2.2% vs 0.5%, P < .001 endometrial).</p><p><strong>Conclusions: </strong>NCCN guidelines missed 65% of cases with P/LP LS variants despite families having higher colorectal and endometrial cancer rates compared with controls. Genomic screening can assist in identifying individuals at risk for LS-related cancers, providing an opportunity to tailor risk management for cancer prevention and early detection.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":" ","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288957/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkaf061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lynch syndrome (LS) is a hereditary cancer predisposition that increases risk for colorectal, endometrial, and other cancers. Although population-based genomic screening programs identify individuals with LS, clinical presentation in such genomically ascertained populations is unknown.
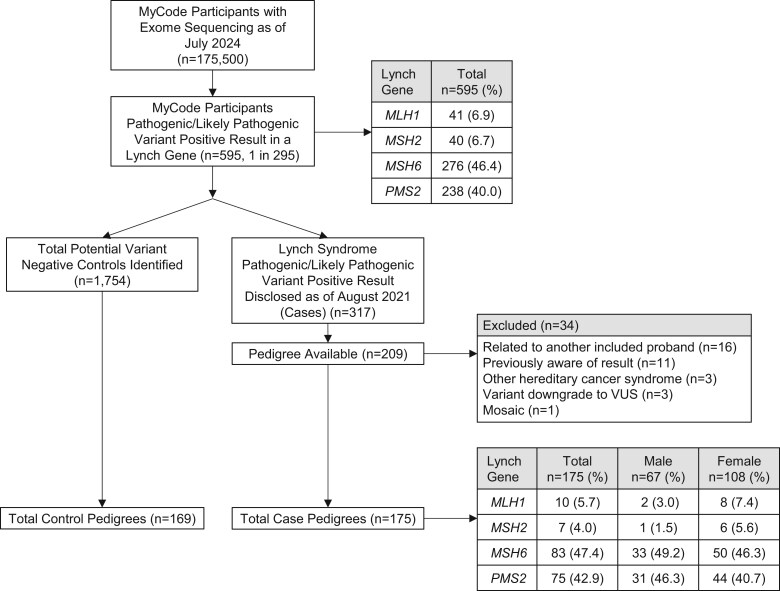
Methods: MyCode is a healthcare system-based biobank that returns clinically actionable genomic screening results to participants, including pathogenic/likely pathogenic (P/LP) variants in LS genes (MLH1, MSH2, MSH6, PMS2). Adult cases (participants with an LS result) and controls (participants without a cancer predisposition variant matched to cases) reported their personal and family cancer histories. Rates of meeting National Comprehensive Cancer Network (NCCN) genetic testing guidelines and rates of colorectal and endometrial cancers in cases, controls, and their family members were calculated and compared.
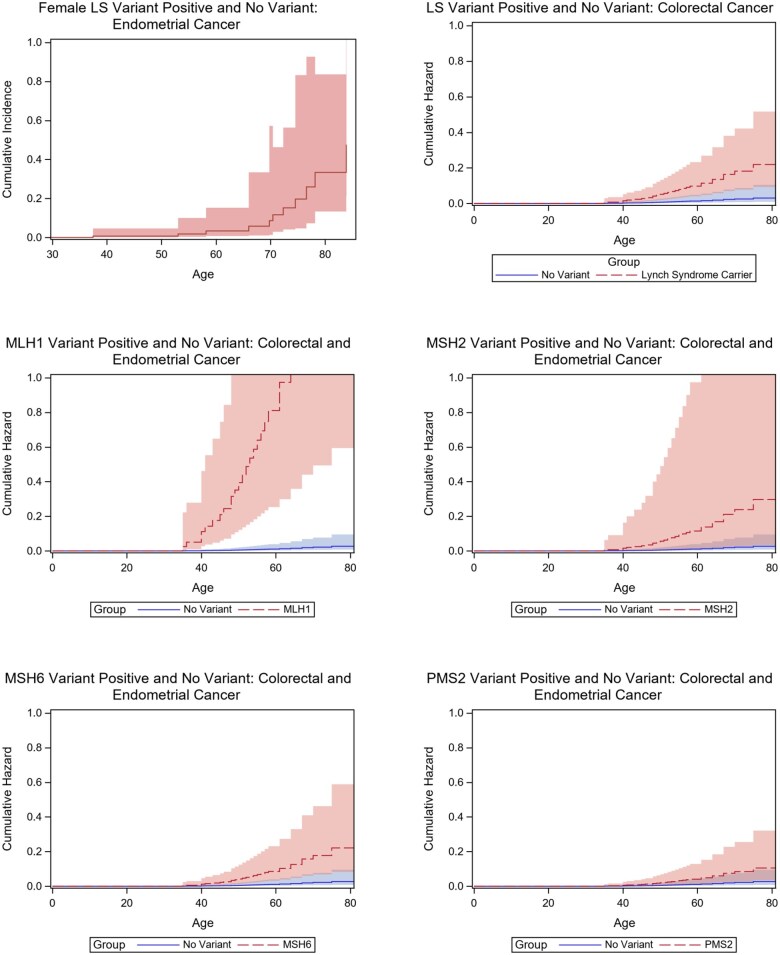
Results: A total of 175 cases (10 MLH1, 7 MSH2, 83 MSH6, and 75 PMS2) and 169 controls were included. Of case pedigrees, 62/175 (35.4%) met NCCN criteria for LS evaluation. Case pedigrees were more likely (P < .001) to meet criteria than control pedigrees (4/169, 8.35%). Case probands had significantly higher rates of colorectal and endometrial cancer than controls (7.7% vs 2.4%, P = .03 colorectal; 11.5% vs 0%, P < .001 endometrial), as did their relatives (3.1% vs 0.9%, P < .001 colorectal; 2.2% vs 0.5%, P < .001 endometrial).
Conclusions: NCCN guidelines missed 65% of cases with P/LP LS variants despite families having higher colorectal and endometrial cancer rates compared with controls. Genomic screening can assist in identifying individuals at risk for LS-related cancers, providing an opportunity to tailor risk management for cancer prevention and early detection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


