{"title":"A Farewell to Arms - An Institutional Review of Conventional Staging for Intermediate-Risk Prostate Cancer.","authors":"Rustam Karanjia, Pallab Sarkar, Vishnu Basavaraju, Oluwabunmi Tayo, Sashi Kommu, Humayun Bashir, Edward Streeter","doi":"10.2478/jcas-2025-0006","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>EAU guidelines advise patients with intermediate risk Gleason 4+3=7 prostate cancer undergo cross-sectional abdominopelvic imaging and bone scan for metastatic screening. We hypothesised detection rate of extra-prostatic disease in this cohort is low using conventional CT/bone scans and could potentially be avoided.</p><p><strong>Materials and methods: </strong>Patients with overall Gleason 4+3 histology were identified over 69 months at East Kent University Hospitals NHS Trust. Patients were excluded if PSA >20ng/mL and/or MRI prostate >T3b stage. Primary outcomes were: (a) detection rates of metastatic disease using conventional CT and bone scan and b) the proportion of fully-staged patients with positive lymph nodes at dissection or biochemical recurrence following robotic-assisted laparoscopic prostatectomy (RALP).</p><p><strong>Results: </strong>A total of 134 patients were identified. Median age was 72 (range 45-83), PSA 7.8ng/mL (range 1.8-19.3) and prostate volume 40cc (range 10-129). 130/134(97%) had MRI scans prior to staging. 124/134(93%) had bone scans and 83/134(62%) had CT scans, of which 77/134(57%) had both. 0/124(0%) bone scans identified metastatic disease and only 2/83(2%) CT scans identified nodal disease not detected by MRI. 0/134(0%) had management changes from staging. 57/134(43%) patients negatively-staged proceeded to RALP. 19/57(32%) had lymph node dissections. 6(11%) had missed metastatic disease at 19 months median follow-up.</p><p><strong>Conclusion: </strong>Detection of metastatic disease by conventional CT and bone scan was poor in this cohort, despite their presence, and their recommendation by EAU seems unwarranted. Patients could safely avoid these scans and proceed directly to radical treatment, due to the theoretical benefit of treating despite oligometastatic disease.</p>","PeriodicalId":73631,"journal":{"name":"Journal of cancer & allied specialties","volume":"11 1","pages":"24-28"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12147702/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cancer & allied specialties","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jcas-2025-0006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: EAU guidelines advise patients with intermediate risk Gleason 4+3=7 prostate cancer undergo cross-sectional abdominopelvic imaging and bone scan for metastatic screening. We hypothesised detection rate of extra-prostatic disease in this cohort is low using conventional CT/bone scans and could potentially be avoided.
Materials and methods: Patients with overall Gleason 4+3 histology were identified over 69 months at East Kent University Hospitals NHS Trust. Patients were excluded if PSA >20ng/mL and/or MRI prostate >T3b stage. Primary outcomes were: (a) detection rates of metastatic disease using conventional CT and bone scan and b) the proportion of fully-staged patients with positive lymph nodes at dissection or biochemical recurrence following robotic-assisted laparoscopic prostatectomy (RALP).
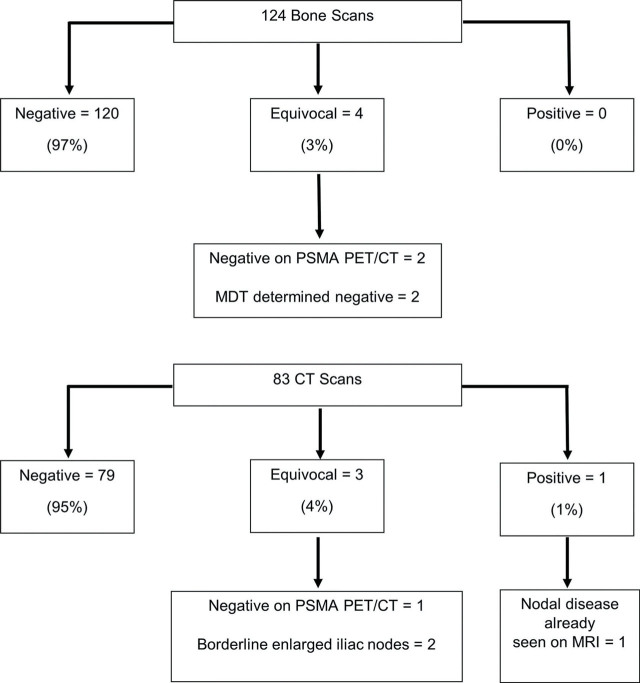
Results: A total of 134 patients were identified. Median age was 72 (range 45-83), PSA 7.8ng/mL (range 1.8-19.3) and prostate volume 40cc (range 10-129). 130/134(97%) had MRI scans prior to staging. 124/134(93%) had bone scans and 83/134(62%) had CT scans, of which 77/134(57%) had both. 0/124(0%) bone scans identified metastatic disease and only 2/83(2%) CT scans identified nodal disease not detected by MRI. 0/134(0%) had management changes from staging. 57/134(43%) patients negatively-staged proceeded to RALP. 19/57(32%) had lymph node dissections. 6(11%) had missed metastatic disease at 19 months median follow-up.
Conclusion: Detection of metastatic disease by conventional CT and bone scan was poor in this cohort, despite their presence, and their recommendation by EAU seems unwarranted. Patients could safely avoid these scans and proceed directly to radical treatment, due to the theoretical benefit of treating despite oligometastatic disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


