Associations of Physical Activity, Sedentary Behaviour, Pain, Function and Quality of Life With Diabetes and Knee Osteoarthritis: Data From the Osteoarthritis Initiative.
Harvi F Hart, Daniel K White, Sonja M Reichert, Joshua J Stefanik
{"title":"Associations of Physical Activity, Sedentary Behaviour, Pain, Function and Quality of Life With Diabetes and Knee Osteoarthritis: Data From the Osteoarthritis Initiative.","authors":"Harvi F Hart, Daniel K White, Sonja M Reichert, Joshua J Stefanik","doi":"10.1002/msc.70128","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the relation of radiographic knee osteoarthritis (RKOA) and type 2 diabetes mellitus (T2DM) to physical activity, pain, physical function, and quality of life.</p><p><strong>Methods: </strong>Data on physical activity (light and moderate-vigorous physical activity minutes/day, steps/day, sedentary time percent of wear time), pain, physical function (Western Ontario and McMaster Index, walking speed during 20-m walk) and quality of life (SF-12) from the Osteoarthritis Initiative at the 48-month visit were included. Participants (n = 1788) were categorised into no RKOA or T2DM, RKOA-alone, T2DM-alone, and RKOA and T2DM. Multivariable regression models, adjusted for age, sex, and BMI, assessed the relationship of disease status to outcomes.</p><p><strong>Results: </strong>Compared to RKOA-alone, RKOA and T2DM were associated with lower moderate-vigorous physical activity (Coefficient: 4 min/day, 95% CI: [-7, -1]) and steps/day (-817 steps/day [-1291, -343]) and higher sedentary time percent (1.3%/day [-0.2, 2.8]). No significant differences were found in light physical activity (-11 min/day [-25, 2]). The RKOA and T2DM groups reported greater pain (1.0 [0.4, 1.6]) and functional limitations (3 [1, 5]), slower walking speed (-0.09 m/s [-0.12, -0.05]), and worse quality of life (-3.2 [-4.8, -1.6]). T2DM-alone was also associated with lower physical activity and worse quality of life than RKOA-alone.</p><p><strong>Conclusions: </strong>The comorbidity of RKOA and T2DM and T2DM-alone were associated with lower physical activity and worse quality of life than RKOA-alone. Management should address both conditions concurrently rather than in isolation.</p>","PeriodicalId":46945,"journal":{"name":"Musculoskeletal Care","volume":"23 2","pages":"e70128"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152236/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Musculoskeletal Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/msc.70128","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate the relation of radiographic knee osteoarthritis (RKOA) and type 2 diabetes mellitus (T2DM) to physical activity, pain, physical function, and quality of life.
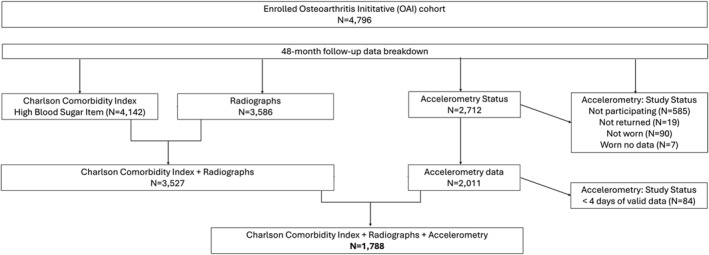
Methods: Data on physical activity (light and moderate-vigorous physical activity minutes/day, steps/day, sedentary time percent of wear time), pain, physical function (Western Ontario and McMaster Index, walking speed during 20-m walk) and quality of life (SF-12) from the Osteoarthritis Initiative at the 48-month visit were included. Participants (n = 1788) were categorised into no RKOA or T2DM, RKOA-alone, T2DM-alone, and RKOA and T2DM. Multivariable regression models, adjusted for age, sex, and BMI, assessed the relationship of disease status to outcomes.
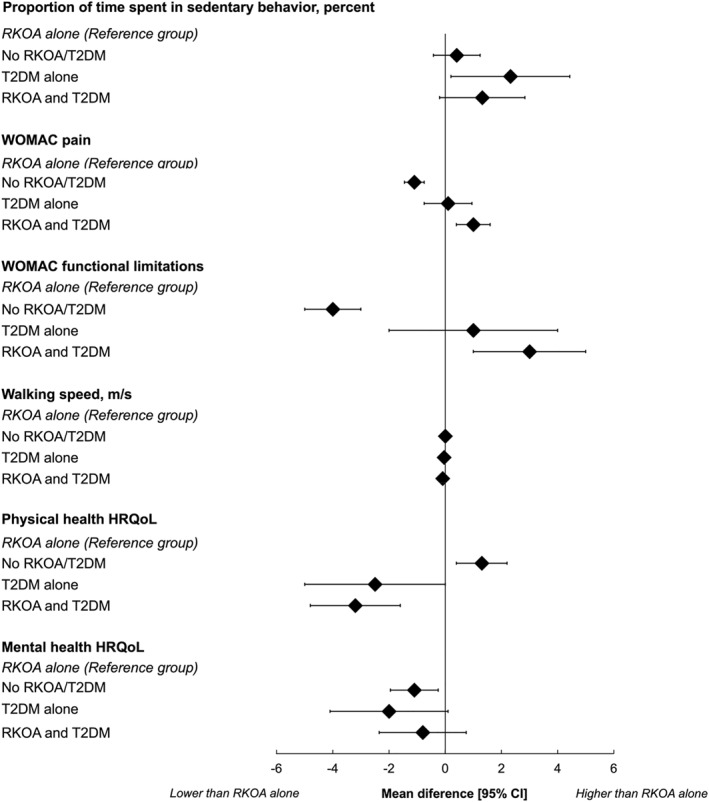
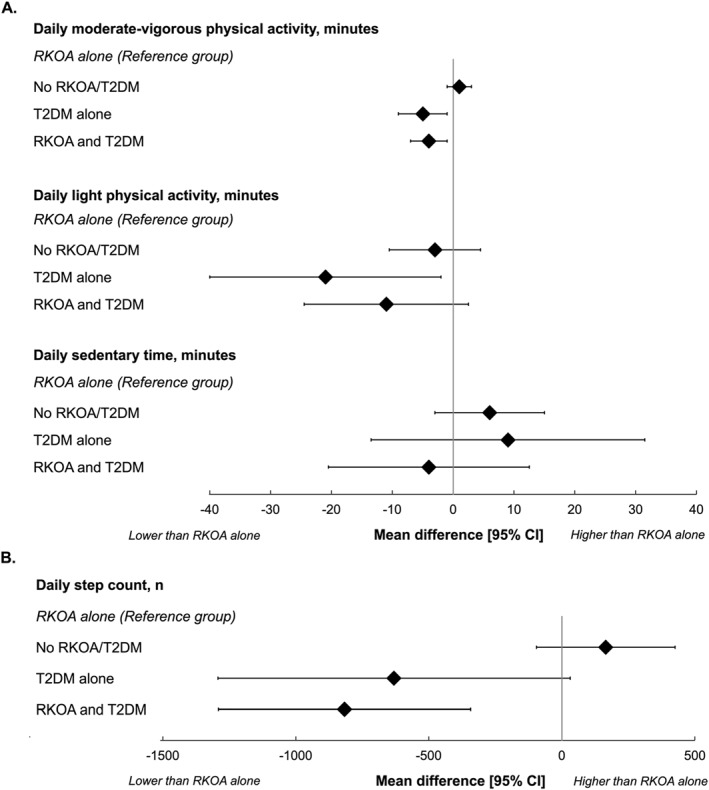
Results: Compared to RKOA-alone, RKOA and T2DM were associated with lower moderate-vigorous physical activity (Coefficient: 4 min/day, 95% CI: [-7, -1]) and steps/day (-817 steps/day [-1291, -343]) and higher sedentary time percent (1.3%/day [-0.2, 2.8]). No significant differences were found in light physical activity (-11 min/day [-25, 2]). The RKOA and T2DM groups reported greater pain (1.0 [0.4, 1.6]) and functional limitations (3 [1, 5]), slower walking speed (-0.09 m/s [-0.12, -0.05]), and worse quality of life (-3.2 [-4.8, -1.6]). T2DM-alone was also associated with lower physical activity and worse quality of life than RKOA-alone.
Conclusions: The comorbidity of RKOA and T2DM and T2DM-alone were associated with lower physical activity and worse quality of life than RKOA-alone. Management should address both conditions concurrently rather than in isolation.
期刊介绍:
Musculoskeletal Care is a peer-reviewed journal for all health professionals committed to the clinical delivery of high quality care for people with musculoskeletal conditions and providing knowledge to support decision making by professionals, patients and policy makers. This journal publishes papers on original research, applied research, review articles and clinical guidelines. Regular topics include patient education, psychological and social impact, patient experiences of health care, clinical up dates and the effectiveness of therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


