Avinaash R Sager, Rupak Desai, Maneeth Mylavarapu, Dipsa Shastri, Nikitha Devaprasad, Shiva N Thiagarajan, Deepak Chandramohan, Anshuman Agrawal, Urmi Gada, Akhil Jain
{"title":"Cannabis use disorder and severe sepsis outcomes in cancer patients: Insights from a national inpatient sample.","authors":"Avinaash R Sager, Rupak Desai, Maneeth Mylavarapu, Dipsa Shastri, Nikitha Devaprasad, Shiva N Thiagarajan, Deepak Chandramohan, Anshuman Agrawal, Urmi Gada, Akhil Jain","doi":"10.5492/wjccm.v14.i2.100844","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The burden of cannabis use disorder (CUD) in the context of its prevalence and subsequent cardiopulmonary outcomes among cancer patients with severe sepsis is unclear.</p><p><strong>Aim: </strong>To address this knowledge gap, especially due to rising patterns of cannabis use and its emerging pharmacological role in cancer.</p><p><strong>Methods: </strong>By applying relevant International Classification of Diseases, Ninth and Tenth Revision, Clinical Modification codes to the National Inpatient Sample database between 2016-2020, we identified CUD(+) and CUD(-) arms among adult cancer admissions with severe sepsis. Comparing the two cohorts, we examined baseline demographic characteristics, epidemiological trends, major adverse cardiac and cerebrovascular events, respiratory failure, hospital cost, and length of stay. We used the Pearson <i>χ</i> <sup>2</sup> d test for categorical variables and the Mann-Whitney <i>U</i> test for continuous, non-normally distributed variables. Multivariable regression analysis was used to control for potential confounders. A <i>P</i> value ≤ 0.05 was considered for statistical significance.</p><p><strong>Results: </strong>We identified a total of 743520 cancer patients admitted with severe sepsis, of which 4945 had CUD. Demographically, the CUD(+) cohort was more likely to be younger (median age = 58 <i>vs</i> 69, <i>P</i> < 0.001), male (67.9% <i>vs</i> 57.2%, <i>P</i> < 0.001), black (23.7% <i>vs</i> 14.4%, <i>P</i> < 0.001), Medicaid enrollees (35.2% <i>vs</i> 10.7%, <i>P</i> < 0.001), in whom higher rates of substance use and depression were observed. CUD(+) patients also exhibited a higher prevalence of chronic pulmonary disease but lower rates of cardiovascular comorbidities. There was no significant difference in major adverse cardiac and cerebrovascular events between CUD(+) and CUD(-) cohorts on multivariable regression analysis. However, the CUD(+) cohort had lower all-cause mortality (adjusted odds ratio = 0.83, 95% confidence interval: 0.7-0.97, <i>P</i> < 0.001) and respiratory failure (adjusted odds ratio = 0.8, 95% confidence interval: 0.69-0.92, <i>P</i> = 0.002). Both groups had similar median length of stay, though CUD(+) patients were more likely to have higher hospital cost compared to CUD(-) patients (median = 94574 dollars <i>vs</i> 86615 dollars, <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>CUD(+) cancer patients with severe sepsis, who tended to be younger, black, males with higher rates of substance use and depression had paradoxically significantly lower odds of all-cause in-hospital mortality and respiratory failure. Future research should aim to better elucidate the underlying mechanisms for these observations.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"14 2","pages":"100844"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11891851/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v14.i2.100844","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The burden of cannabis use disorder (CUD) in the context of its prevalence and subsequent cardiopulmonary outcomes among cancer patients with severe sepsis is unclear.
Aim: To address this knowledge gap, especially due to rising patterns of cannabis use and its emerging pharmacological role in cancer.
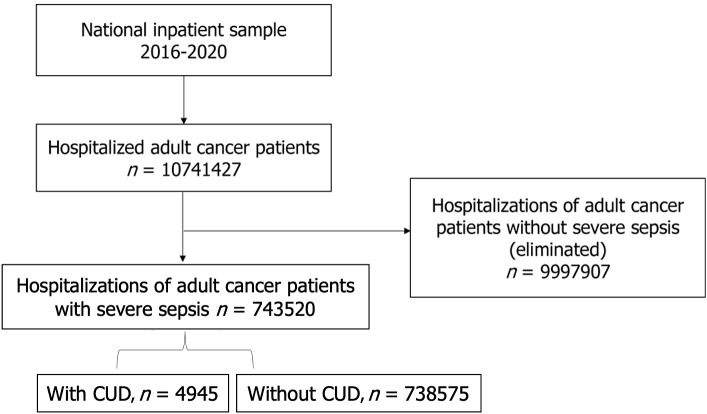
Methods: By applying relevant International Classification of Diseases, Ninth and Tenth Revision, Clinical Modification codes to the National Inpatient Sample database between 2016-2020, we identified CUD(+) and CUD(-) arms among adult cancer admissions with severe sepsis. Comparing the two cohorts, we examined baseline demographic characteristics, epidemiological trends, major adverse cardiac and cerebrovascular events, respiratory failure, hospital cost, and length of stay. We used the Pearson χ2 d test for categorical variables and the Mann-Whitney U test for continuous, non-normally distributed variables. Multivariable regression analysis was used to control for potential confounders. A P value ≤ 0.05 was considered for statistical significance.
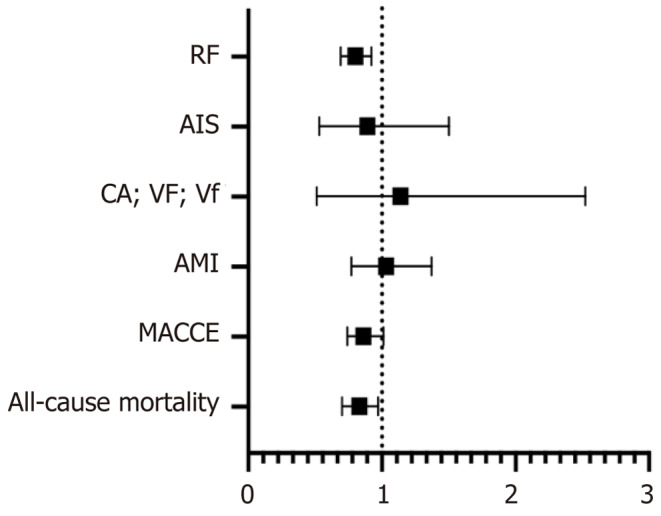
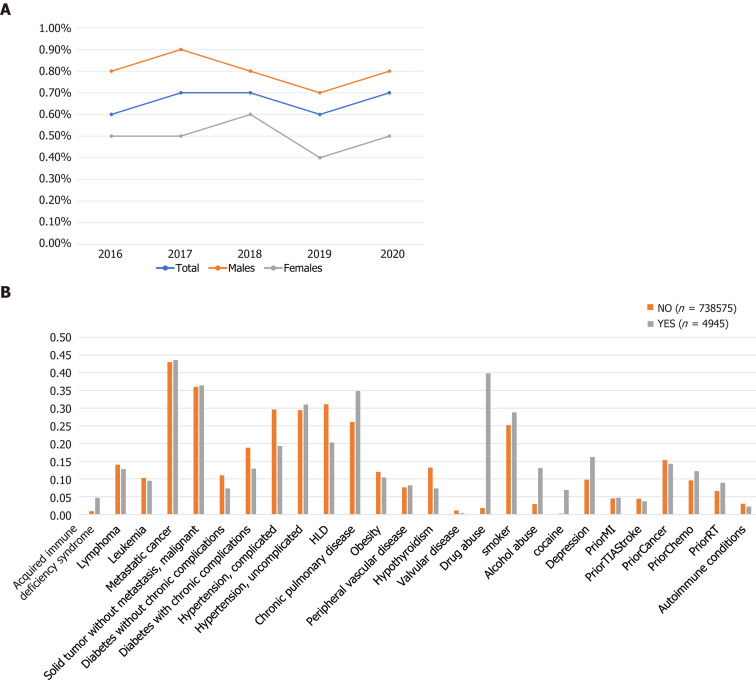
Results: We identified a total of 743520 cancer patients admitted with severe sepsis, of which 4945 had CUD. Demographically, the CUD(+) cohort was more likely to be younger (median age = 58 vs 69, P < 0.001), male (67.9% vs 57.2%, P < 0.001), black (23.7% vs 14.4%, P < 0.001), Medicaid enrollees (35.2% vs 10.7%, P < 0.001), in whom higher rates of substance use and depression were observed. CUD(+) patients also exhibited a higher prevalence of chronic pulmonary disease but lower rates of cardiovascular comorbidities. There was no significant difference in major adverse cardiac and cerebrovascular events between CUD(+) and CUD(-) cohorts on multivariable regression analysis. However, the CUD(+) cohort had lower all-cause mortality (adjusted odds ratio = 0.83, 95% confidence interval: 0.7-0.97, P < 0.001) and respiratory failure (adjusted odds ratio = 0.8, 95% confidence interval: 0.69-0.92, P = 0.002). Both groups had similar median length of stay, though CUD(+) patients were more likely to have higher hospital cost compared to CUD(-) patients (median = 94574 dollars vs 86615 dollars, P < 0.001).
Conclusion: CUD(+) cancer patients with severe sepsis, who tended to be younger, black, males with higher rates of substance use and depression had paradoxically significantly lower odds of all-cause in-hospital mortality and respiratory failure. Future research should aim to better elucidate the underlying mechanisms for these observations.
背景:大麻使用障碍(CUD)在严重脓毒症癌症患者的患病率和随后的心肺结局方面的负担尚不清楚。目的:解决这一知识差距,特别是由于大麻使用模式的增加及其在癌症中的新药理作用。方法:将相关的《国际疾病分类》第九版和第十版临床修改代码应用于2016-2020年全国住院患者样本数据库,对成人癌症住院严重脓毒症患者的CUD(+)和CUD(-)臂进行鉴定。比较两个队列,我们检查了基线人口统计学特征、流行病学趋势、主要不良心脑血管事件、呼吸衰竭、住院费用和住院时间。我们对分类变量使用Pearson χ 2检验,对连续、非正态分布变量使用Mann-Whitney U检验。采用多变量回归分析控制潜在混杂因素。以P值≤0.05为有统计学意义。结果:我们共确定了743520例因严重脓毒症入院的癌症患者,其中4945例患有CUD。人口统计学上,CUD(+)队列更可能是年轻人(中位年龄= 58 vs 69, P < 0.001)、男性(67.9% vs 57.2%, P < 0.001)、黑人(23.7% vs 14.4%, P < 0.001)、医疗补助计划参保者(35.2% vs 10.7%, P < 0.001),在这些人群中观察到较高的物质使用和抑郁率。CUD(+)患者还表现出更高的慢性肺部疾病患病率,但心血管合并症的发生率较低。多变量回归分析显示,CUD(+)组与CUD(-)组的主要心脑血管不良事件发生率无显著差异。然而,CUD(+)队列的全因死亡率(校正优势比= 0.83,95%可信区间:0.7-0.97,P < 0.001)和呼吸衰竭(校正优势比= 0.8,95%可信区间:0.69-0.92,P = 0.002)较低。两组患者的平均住院时间相似,尽管CUD(+)患者比CUD(-)患者更可能有更高的住院费用(中位数= 94574美元对86615美元,P < 0.001)。结论:CUD(+)癌症患者合并严重脓毒症,往往是年轻、黑人、男性,物质使用和抑郁率较高,其全因住院死亡率和呼吸衰竭的几率显着显著降低。未来的研究应旨在更好地阐明这些观察的潜在机制。
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


