{"title":"Dexmedetomidine and acute kidney injury in patients with sepsis: a retrospective cohort study.","authors":"Papawadee Chaengsuthiworawat, Tharin Thampongsa, Thanyalak Thamjamrassri, Chawika Pisitsak","doi":"10.1007/s12630-025-02977-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Acute kidney injury (AKI) is a common complication of sepsis. AKI is associated with increased morbidity and mortality. Studies show that dexmedetomidine has a protective effect against AKI. We sought to evaluate the association between dexmedetomidine administration and AKI in patients with sepsis.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of 331 adult patients with sepsis. We divided patients into two groups: patients who received an infusion of dexmedetomidine of ≥ 0.2 µg·kg<sup>-1</sup>·hr<sup>-1</sup> for > 6 hr within 72 hr of sepsis diagnosis (the dexmedetomidine group; N = 73) and patients who did not receive a dexmedetomidine infusion (the nondexmedetomidine group; N = 258). The primary outcome was the incidence of AKI within seven days, defined by the Kidney Disease Improving Global Outcomes (KDIGO) criteria. We analyzed our results using multivariable logistic regression models including 1) the entire cohort (331 patients) or 2) a 1:1 propensity-score-matched cohort (73 patients per group).</p><p><strong>Results: </strong>Acute kidney injury was diagnosed in 190/331 (57.4%) patients. The incidence of AKI was not different between the dexmedetomidine group and the nondexmedetomidine group in both the entire cohort (54.8% vs 58.1%; P = 0.61) and the propensity-matched cohort (54.7% vs 63.0%; P = 0.31). Additionally, there were no significant differences between groups in the incidence of renal replacement therapy (10.9% vs 13.6%; P = 0.61) and 30-day mortality (32.8% vs 24.6%; P = 0.27). We observed a statistically significant interaction between patient age > 65 yr and reduced odds of developing AKI in patients who received dexmedetomidine (adjusted odds ratio, 0.25; 95% confidence interval, 0.07 to 0.90; P = 0.03).</p><p><strong>Conclusions: </strong>While there was no association between dexmedetomidine administration and AKI in our overall cohort of patients with sepsis, we observed reduced odds of developing AKI in older patients (aged > 65 yr) who received dexmedetomidine. Further research is needed to confirm that dexmedetomidine has a protective effect against AKI in this patient population.</p>","PeriodicalId":56145,"journal":{"name":"Canadian Journal of Anesthesia-Journal Canadien D Anesthesie","volume":" ","pages":"966-974"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12228650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Anesthesia-Journal Canadien D Anesthesie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12630-025-02977-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Acute kidney injury (AKI) is a common complication of sepsis. AKI is associated with increased morbidity and mortality. Studies show that dexmedetomidine has a protective effect against AKI. We sought to evaluate the association between dexmedetomidine administration and AKI in patients with sepsis.
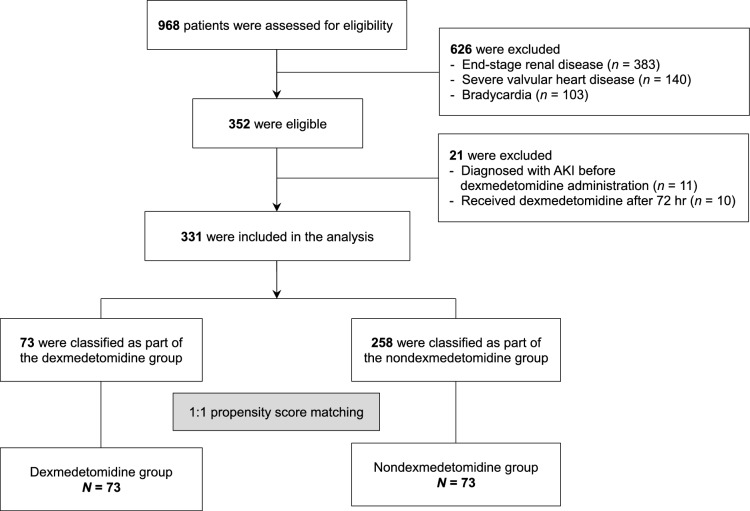
Methods: We conducted a retrospective cohort study of 331 adult patients with sepsis. We divided patients into two groups: patients who received an infusion of dexmedetomidine of ≥ 0.2 µg·kg-1·hr-1 for > 6 hr within 72 hr of sepsis diagnosis (the dexmedetomidine group; N = 73) and patients who did not receive a dexmedetomidine infusion (the nondexmedetomidine group; N = 258). The primary outcome was the incidence of AKI within seven days, defined by the Kidney Disease Improving Global Outcomes (KDIGO) criteria. We analyzed our results using multivariable logistic regression models including 1) the entire cohort (331 patients) or 2) a 1:1 propensity-score-matched cohort (73 patients per group).
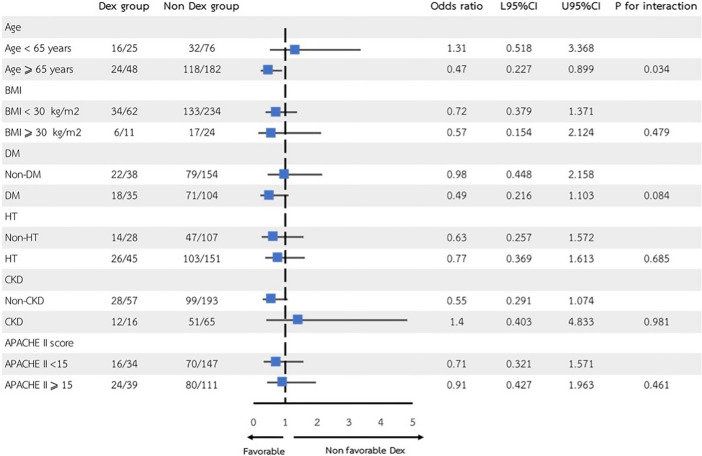
Results: Acute kidney injury was diagnosed in 190/331 (57.4%) patients. The incidence of AKI was not different between the dexmedetomidine group and the nondexmedetomidine group in both the entire cohort (54.8% vs 58.1%; P = 0.61) and the propensity-matched cohort (54.7% vs 63.0%; P = 0.31). Additionally, there were no significant differences between groups in the incidence of renal replacement therapy (10.9% vs 13.6%; P = 0.61) and 30-day mortality (32.8% vs 24.6%; P = 0.27). We observed a statistically significant interaction between patient age > 65 yr and reduced odds of developing AKI in patients who received dexmedetomidine (adjusted odds ratio, 0.25; 95% confidence interval, 0.07 to 0.90; P = 0.03).
Conclusions: While there was no association between dexmedetomidine administration and AKI in our overall cohort of patients with sepsis, we observed reduced odds of developing AKI in older patients (aged > 65 yr) who received dexmedetomidine. Further research is needed to confirm that dexmedetomidine has a protective effect against AKI in this patient population.
期刊介绍:
The Canadian Journal of Anesthesia (the Journal) is owned by the Canadian Anesthesiologists’
Society and is published by Springer Science + Business Media, LLM (New York). From the
first year of publication in 1954, the international exposure of the Journal has broadened
considerably, with articles now received from over 50 countries. The Journal is published
monthly, and has an impact Factor (mean journal citation frequency) of 2.127 (in 2012). Article
types consist of invited editorials, reports of original investigations (clinical and basic sciences
articles), case reports/case series, review articles, systematic reviews, accredited continuing
professional development (CPD) modules, and Letters to the Editor. The editorial content,
according to the mission statement, spans the fields of anesthesia, acute and chronic pain,
perioperative medicine and critical care. In addition, the Journal publishes practice guidelines
and standards articles relevant to clinicians. Articles are published either in English or in French,
according to the language of submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


