Chirag Soni, Victor Koltenyuk, Nithin Gupta, Haad A Arif, Aruni Areti, Taylor Manes, Luke A Lopas, Jan P Szatkowski, Christian A Bowers, Benjamin C Taylor, Jack W Weick
{"title":"Utility of Revised Risk Analysis Index as a Predictor of Mortality and Morbidity in Orthopaedic Trauma.","authors":"Chirag Soni, Victor Koltenyuk, Nithin Gupta, Haad A Arif, Aruni Areti, Taylor Manes, Luke A Lopas, Jan P Szatkowski, Christian A Bowers, Benjamin C Taylor, Jack W Weick","doi":"10.5435/JAAOSGlobal-D-25-00086","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to determine the applicability of the Revised Risk Analysis Index (RAI-Rev) in orthopaedic trauma and compare the predictive discrimination for the RAI-Rev and the 5-Item Modified Frailty Index (mFI-5) for 30-day postoperative outcomes.</p><p><strong>Methods: </strong></p><p><strong>Design: </strong>This is a retrospective cohort study.</p><p><strong>Setting: </strong>The American College of Surgeons National Surgical Quality Improvement database was used.</p><p><strong>Patient selection: </strong>All patients aged 18 or older who underwent surgical treatment for forearm, humerus, pelvis, acetabulum, femur, tibia, and hindfoot fractures from 2015 to 2020 were included.</p><p><strong>Outcome: </strong>30-day postoperative mortality, major complications, and wound complications consisting of surgical site infection, and wound dehiscence were measured.</p><p><strong>Results: </strong>A total of 206,352 patients met inclusion criteria. The mean age was 69 years, with 64.2% (n = 132,514) being female. Multivariate regression analysis showed that increasing frailty tiers in both RAI-Rev and mFI-5 were independent predictors of mortality, major complications, readmission, and wound complications. The cohort with the highest degree of frailty in both RAI-Rev and mFI-5 had the greatest risk of poor outcomes. RAI-Rev had significantly superior predictive discriminatory thresholds compared with mFI-5 for predicting 30-day mortality (C-statistic: RAI-Rev [0.84] and mFI-5 [0.67], P < 0.001), major complications (C-statistic: RAI-Rev [0.73] and mFI-5 [0.65], P < 0.001), and readmission (C-statistic: RAI-Rev [0.68] and mFI-5 [0.63], P < 0.001). However, mFI-5 outperformed RAI-Rev when predicting wound complications (C-statistic: RAI-Rev [0.52] and mFI-5 [0.55], P < 0.001).</p><p><strong>Conclusion: </strong>The RAI-Rev tool demonstrated superior predictability of postoperative morbidity, mortality, and readmission rates compared with mFI-5 but was less effective in predicting surgical site complications. These findings demonstrate the utility of RAI-Rev in anticipating postoperative complications in the setting of orthopaedic trauma, where optimizing surgical candidate selection is not always possible. Assessing the predicted morbidity and mortality through RAI-Rev enables surgeons to accurately identify patients at high risk of complications, which can further research investigation to mitigate this risk.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 6","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142732/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-25-00086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The aim of this study was to determine the applicability of the Revised Risk Analysis Index (RAI-Rev) in orthopaedic trauma and compare the predictive discrimination for the RAI-Rev and the 5-Item Modified Frailty Index (mFI-5) for 30-day postoperative outcomes.
Methods:
Design: This is a retrospective cohort study.
Setting: The American College of Surgeons National Surgical Quality Improvement database was used.
Patient selection: All patients aged 18 or older who underwent surgical treatment for forearm, humerus, pelvis, acetabulum, femur, tibia, and hindfoot fractures from 2015 to 2020 were included.
Outcome: 30-day postoperative mortality, major complications, and wound complications consisting of surgical site infection, and wound dehiscence were measured.
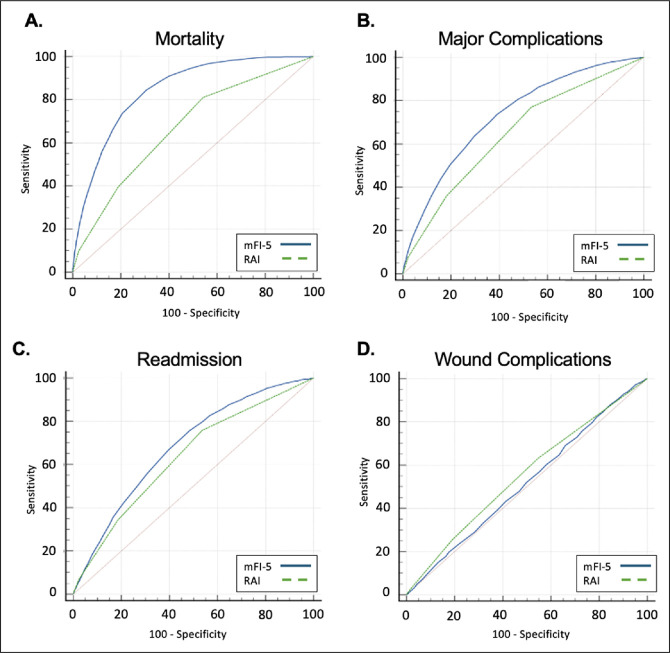
Results: A total of 206,352 patients met inclusion criteria. The mean age was 69 years, with 64.2% (n = 132,514) being female. Multivariate regression analysis showed that increasing frailty tiers in both RAI-Rev and mFI-5 were independent predictors of mortality, major complications, readmission, and wound complications. The cohort with the highest degree of frailty in both RAI-Rev and mFI-5 had the greatest risk of poor outcomes. RAI-Rev had significantly superior predictive discriminatory thresholds compared with mFI-5 for predicting 30-day mortality (C-statistic: RAI-Rev [0.84] and mFI-5 [0.67], P < 0.001), major complications (C-statistic: RAI-Rev [0.73] and mFI-5 [0.65], P < 0.001), and readmission (C-statistic: RAI-Rev [0.68] and mFI-5 [0.63], P < 0.001). However, mFI-5 outperformed RAI-Rev when predicting wound complications (C-statistic: RAI-Rev [0.52] and mFI-5 [0.55], P < 0.001).
Conclusion: The RAI-Rev tool demonstrated superior predictability of postoperative morbidity, mortality, and readmission rates compared with mFI-5 but was less effective in predicting surgical site complications. These findings demonstrate the utility of RAI-Rev in anticipating postoperative complications in the setting of orthopaedic trauma, where optimizing surgical candidate selection is not always possible. Assessing the predicted morbidity and mortality through RAI-Rev enables surgeons to accurately identify patients at high risk of complications, which can further research investigation to mitigate this risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


