{"title":"Minimally Invasive L5-S1 Anterior TLIF Cage Placement in Lateral ALIF Exposure as a Bailout Option for Low Iliocaval Junctions: Report of Four Cases.","authors":"Timothy Y Kim, Martin H Pham","doi":"10.1055/s-0045-1806728","DOIUrl":null,"url":null,"abstract":"<p><p>The aim of this study was to demonstrate that anteriorly placed transforaminal lumbar interbody fusion (TLIF) footprint bullet cage is a safe and effective bailout option if difficult left common iliac vein (LCIV) anatomy is unexpectedly encountered during the L5-S1 lateral anterior lumbar interbody fusion (L-ALIF). This retrospective case series includes four patients who received anteriorly placed TLIF cages at L5-S1 during L-ALIF surgery. Demographics, complications, and clinical/radiographic results were collected. The analysis included four female patients with a mean age of 59.0 years and mean body mass index (BMI) of 23.9. Three patients had degenerative conditions and one patient had a deformity. All the patients had an LCIV obstructing the center of the L5-S1 disk space, and titanium TLIF bullet cages were placed and secured with washers and screws. The L5-S1 segmental lordosis increased by 8.3 ± 6.1 degrees with a final mean lordosis of 23.5 ± 8.4 degrees; the L5-S1 intradiskal angle increased by 12.0 ± 7.0 degrees with a final mean disk angle of 18.8 ± 7.0 degrees; the posterior disk height increased by 4.4 ± 2.7 mm with a final mean disk height of 8.0 ± 2.1 mm. The mean numerical rating scale (NRS) for back pain improved by 5.3 ± 2.5 and the mean NRS leg pain improved by 7.7 ± 2.5 over a mean follow-up of 14 months (range: 6-20). There have been no perioperative complications or implant failure to date. If challenging vascular anatomy is encountered during L-ALIF exposure that prevents ALIF footprint cage placement, proceeding with smaller TLIF bullet cage placement anteriorly rather than abandoning the surgical approach is a safe and effective option.</p>","PeriodicalId":94300,"journal":{"name":"Asian journal of neurosurgery","volume":"20 2","pages":"417-422"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136957/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian journal of neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1806728","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
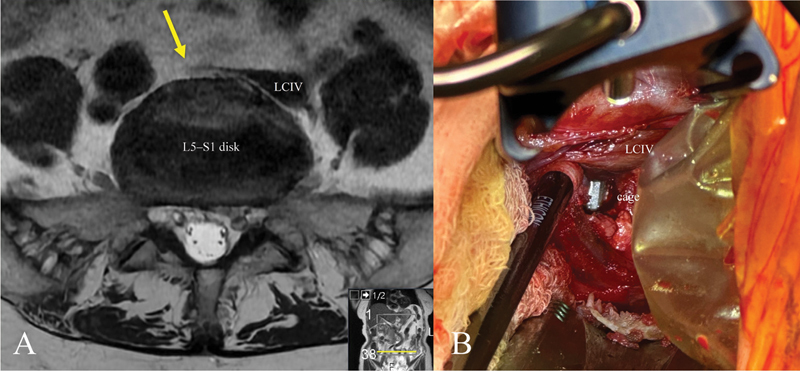
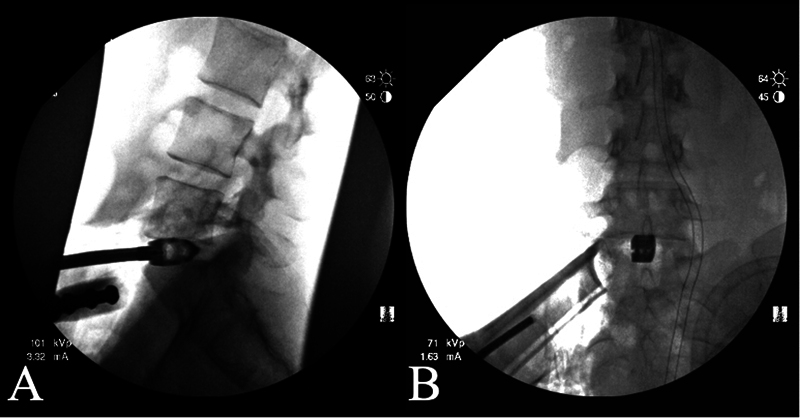
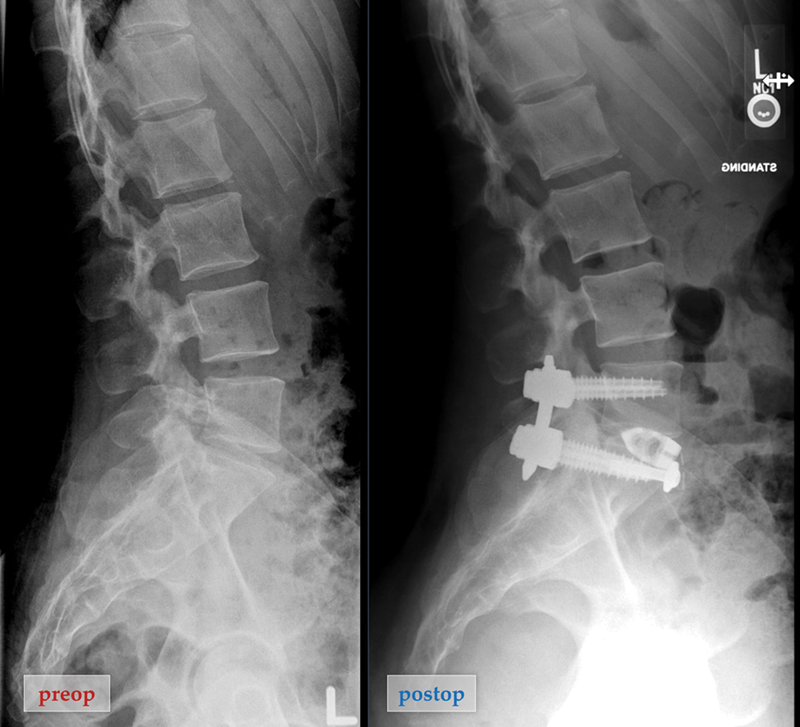
The aim of this study was to demonstrate that anteriorly placed transforaminal lumbar interbody fusion (TLIF) footprint bullet cage is a safe and effective bailout option if difficult left common iliac vein (LCIV) anatomy is unexpectedly encountered during the L5-S1 lateral anterior lumbar interbody fusion (L-ALIF). This retrospective case series includes four patients who received anteriorly placed TLIF cages at L5-S1 during L-ALIF surgery. Demographics, complications, and clinical/radiographic results were collected. The analysis included four female patients with a mean age of 59.0 years and mean body mass index (BMI) of 23.9. Three patients had degenerative conditions and one patient had a deformity. All the patients had an LCIV obstructing the center of the L5-S1 disk space, and titanium TLIF bullet cages were placed and secured with washers and screws. The L5-S1 segmental lordosis increased by 8.3 ± 6.1 degrees with a final mean lordosis of 23.5 ± 8.4 degrees; the L5-S1 intradiskal angle increased by 12.0 ± 7.0 degrees with a final mean disk angle of 18.8 ± 7.0 degrees; the posterior disk height increased by 4.4 ± 2.7 mm with a final mean disk height of 8.0 ± 2.1 mm. The mean numerical rating scale (NRS) for back pain improved by 5.3 ± 2.5 and the mean NRS leg pain improved by 7.7 ± 2.5 over a mean follow-up of 14 months (range: 6-20). There have been no perioperative complications or implant failure to date. If challenging vascular anatomy is encountered during L-ALIF exposure that prevents ALIF footprint cage placement, proceeding with smaller TLIF bullet cage placement anteriorly rather than abandoning the surgical approach is a safe and effective option.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


