{"title":"Tyrosine kinase inhibitor-related factors pre-disposing to post-transplant thrombotic microangiopathy in patients with CML and Ph+ acute leukemias.","authors":"Sachin Punatar, Komal Kumbhalwar, Siddhesh A Kalantri, Anant Gokarn, Lingaraj Nayak, Akanksha Chichra, Sumeet Mirgh, Nishant Jindal, Libin Mathew, Sadhana Kannan, Navin Khattry","doi":"10.31547/bct-2024-029","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We have previously reported that pre-transplant use of tyrosine kinase inhibitors (TKIs) is independently associated with the occurrence of transplant-associated thrombotic microangiopathy (TA-TMA). However, the precise TKI-related factors which predispose to TA-TMA are unknown. In this retrospective analysis, we identify the TKI-related factors that are associated with TA-TMA.</p><p><strong>Methods: </strong>This was a single center retrospective analysis of all patients with Philadelphia chromosome-positive (Ph+) malignancies who received BCR-ABL TKIs prior to transplant and underwent allogeneic hematopoietic stem cell transplantation (HSCT) between January 2008 and March 2019. Definite TA-TMA was defined as per Blood & Marrow Transplant Clinical Trials Network (BMT CTN) criteria and probable TMA as per Cho criteria. Details about the timing of the start and stop of TKI pre-transplant, the dose of TKIs used, and the number of TKIs exposed to pre-transplant were obtained. Imatinib > 400 mg/day, dasatinib > 100 mg/day, or nilotinib > 800 mg/day were considered as high dose TKI.</p><p><strong>Results: </strong>Seventy-two patients with chronic myeloid leukemia (CML)/Ph+ acute leukemias underwent transplant in the above period. Patient, donor, and transplant characteristics are shown in Table 1 and were well-matched between those with and without TMA. Overall, 13 (18%) had TA-TMA (median day +128), with 9 definite and 4 probable. The only TKI-related factor significantly associated with TA-TMA was the use of high-dose TKI (<i>p</i>=0.04). Among non-TKI-related factors, acute graft versus host disease (GVHD) was associated with TA-TMA (<i>p</i>=0.01). On multivariate analysis, high dose TKI did not remain statistically significant (Odds Ratio (OR) 4.6, <i>p</i>=0.16). TA-TMA was associated with significantly worse long-term survival (6-year survival was 30% with TMA versus 62% without TMA, <i>p</i>=0.026).</p><p><strong>Conclusions: </strong>Pre-transplant use of TKI was associated with risk of TMA in about one-fifth of patients. High-dose TKI and acute GVHD increased the risk of TA-TMA. Prospective studies are warranted to confirm these findings. TA-TMA was associated with significantly worse long-term survival.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"8 2","pages":"210-216"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138228/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2024-029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We have previously reported that pre-transplant use of tyrosine kinase inhibitors (TKIs) is independently associated with the occurrence of transplant-associated thrombotic microangiopathy (TA-TMA). However, the precise TKI-related factors which predispose to TA-TMA are unknown. In this retrospective analysis, we identify the TKI-related factors that are associated with TA-TMA.
Methods: This was a single center retrospective analysis of all patients with Philadelphia chromosome-positive (Ph+) malignancies who received BCR-ABL TKIs prior to transplant and underwent allogeneic hematopoietic stem cell transplantation (HSCT) between January 2008 and March 2019. Definite TA-TMA was defined as per Blood & Marrow Transplant Clinical Trials Network (BMT CTN) criteria and probable TMA as per Cho criteria. Details about the timing of the start and stop of TKI pre-transplant, the dose of TKIs used, and the number of TKIs exposed to pre-transplant were obtained. Imatinib > 400 mg/day, dasatinib > 100 mg/day, or nilotinib > 800 mg/day were considered as high dose TKI.
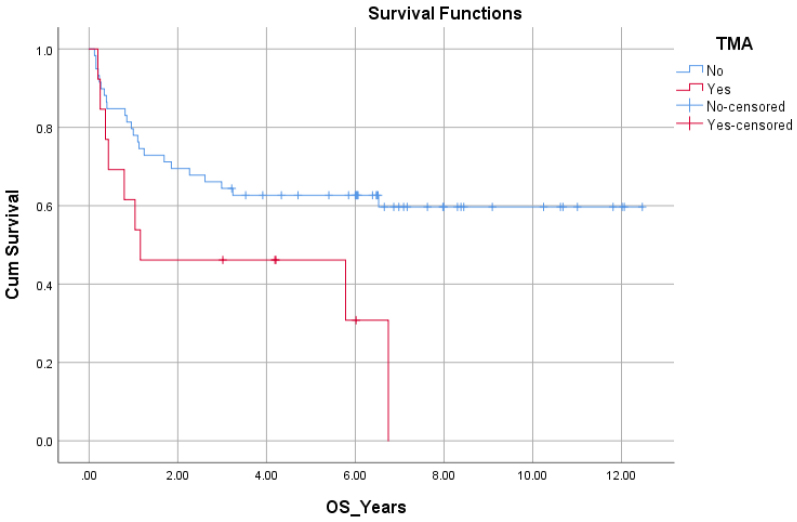
Results: Seventy-two patients with chronic myeloid leukemia (CML)/Ph+ acute leukemias underwent transplant in the above period. Patient, donor, and transplant characteristics are shown in Table 1 and were well-matched between those with and without TMA. Overall, 13 (18%) had TA-TMA (median day +128), with 9 definite and 4 probable. The only TKI-related factor significantly associated with TA-TMA was the use of high-dose TKI (p=0.04). Among non-TKI-related factors, acute graft versus host disease (GVHD) was associated with TA-TMA (p=0.01). On multivariate analysis, high dose TKI did not remain statistically significant (Odds Ratio (OR) 4.6, p=0.16). TA-TMA was associated with significantly worse long-term survival (6-year survival was 30% with TMA versus 62% without TMA, p=0.026).
Conclusions: Pre-transplant use of TKI was associated with risk of TMA in about one-fifth of patients. High-dose TKI and acute GVHD increased the risk of TA-TMA. Prospective studies are warranted to confirm these findings. TA-TMA was associated with significantly worse long-term survival.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


