Kavantissa M Keppetipola, Adam Leibold, Jay Trivedi, Ashmal Sami Kabani, Advith Sarikonda, D Mitchell Self, Emily L Isch, Steven Glener, Srinivas Prasad, Jack Jallo, Joshua E Heller, James Harrop, Alexander R Vaccaro, Ahilan Sivaganesan
{"title":"Time-Driven Activity-Based Costing for Cervical Myelopathy Surgery: A Step Towards Total Episode Costs.","authors":"Kavantissa M Keppetipola, Adam Leibold, Jay Trivedi, Ashmal Sami Kabani, Advith Sarikonda, D Mitchell Self, Emily L Isch, Steven Glener, Srinivas Prasad, Jack Jallo, Joshua E Heller, James Harrop, Alexander R Vaccaro, Ahilan Sivaganesan","doi":"10.2147/CEOR.S502217","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Time-driven activity-based costing (TDABC) is a highly accurate method for determining the true cost of delivering a healthcare service. However, TDABC is most often applied to a singular phase of care such as an outpatient visit or a surgical event. Here we broaden the scope by using TDABC to estimate the costs of surgically treating cervical myelopathy - from the moment of surgical scheduling until post-operative hospital discharge.</p><p><strong>Methods: </strong>In a single-center retrospective study at a large tertiary academic institution, TDABC was employed to measure pre-operative, intra-operative, and post-operative (inpatient) costs for 63 patients undergoing elective surgery for cervical myelopathy. Cost patterns among different surgical approaches (anterior, posterior, anterior/posterior) were analyzed using generalized linear models and the Kruskal-Wallis test.</p><p><strong>Results: </strong>63 consecutive patients who underwent elective surgery for cervical myelopathy were examined (anterior approach: 36.5%, n=23; posterior approach: 54.0%, n=34; anterior/posterior approach: 9.5%, n=6). The average pre-operative, intraoperative, and postoperative costs were $352.83 ± $205, $10,809.09 ± $6052.69, and $5327.07 ± $5114.78, respectively. The average total episode cost for all cases was $16,488.99 ± $8,181,777. Kruskal-Wallis analysis revealed that total episode cost for the anterior-posterior approach was significantly higher than for both the anterior (p<0.001) and posterior approaches (p<0.05), while the total episode cost for the anterior approach was significantly less than that of the posterior (p<0.001).</p><p><strong>Conclusion: </strong>We have demonstrated the feasibility of TDABC for estimating a large fraction of total episode costs for the surgical treatment of cervical myelopathy. This may also be the first attempt at understanding episode costs across multiple surgical options for a given spinal diagnosis, which will be relevant as condition-based bundled payments emerge. As expected, anterior cervical surgeries incurred lower costs than posterior surgeries, which incurred lower costs than anterior-posterior surgeries.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"419-428"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12145145/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S502217","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Time-driven activity-based costing (TDABC) is a highly accurate method for determining the true cost of delivering a healthcare service. However, TDABC is most often applied to a singular phase of care such as an outpatient visit or a surgical event. Here we broaden the scope by using TDABC to estimate the costs of surgically treating cervical myelopathy - from the moment of surgical scheduling until post-operative hospital discharge.
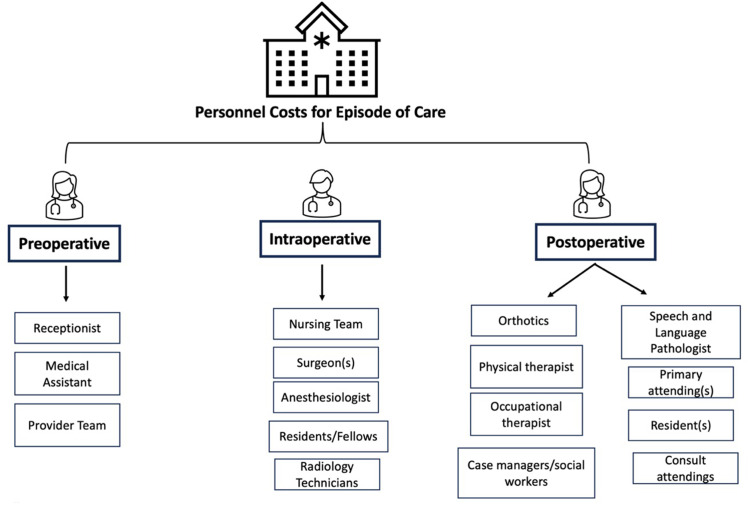
Methods: In a single-center retrospective study at a large tertiary academic institution, TDABC was employed to measure pre-operative, intra-operative, and post-operative (inpatient) costs for 63 patients undergoing elective surgery for cervical myelopathy. Cost patterns among different surgical approaches (anterior, posterior, anterior/posterior) were analyzed using generalized linear models and the Kruskal-Wallis test.
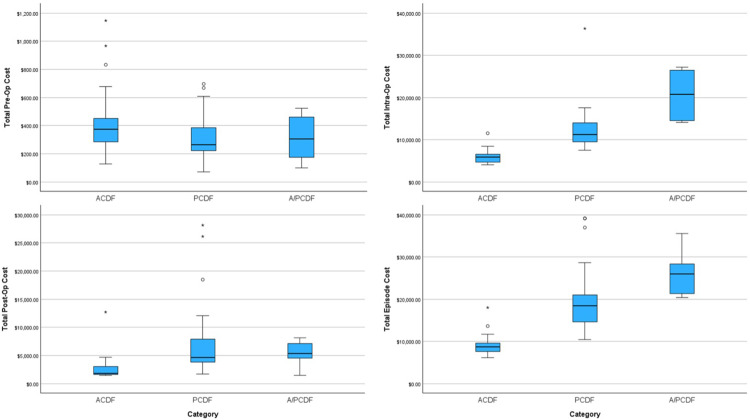
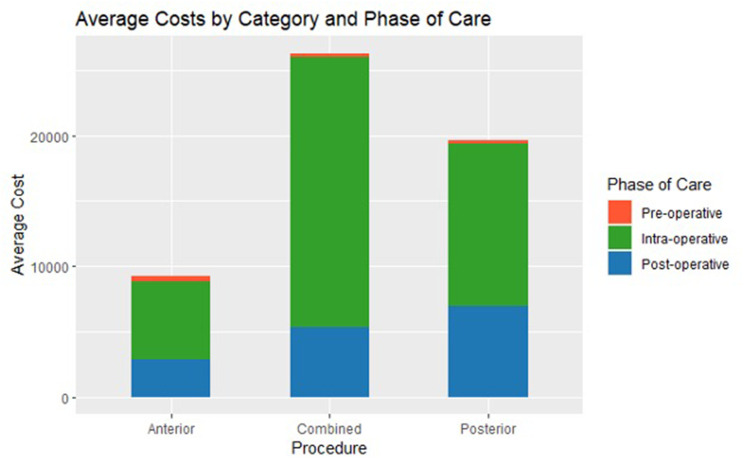
Results: 63 consecutive patients who underwent elective surgery for cervical myelopathy were examined (anterior approach: 36.5%, n=23; posterior approach: 54.0%, n=34; anterior/posterior approach: 9.5%, n=6). The average pre-operative, intraoperative, and postoperative costs were $352.83 ± $205, $10,809.09 ± $6052.69, and $5327.07 ± $5114.78, respectively. The average total episode cost for all cases was $16,488.99 ± $8,181,777. Kruskal-Wallis analysis revealed that total episode cost for the anterior-posterior approach was significantly higher than for both the anterior (p<0.001) and posterior approaches (p<0.05), while the total episode cost for the anterior approach was significantly less than that of the posterior (p<0.001).
Conclusion: We have demonstrated the feasibility of TDABC for estimating a large fraction of total episode costs for the surgical treatment of cervical myelopathy. This may also be the first attempt at understanding episode costs across multiple surgical options for a given spinal diagnosis, which will be relevant as condition-based bundled payments emerge. As expected, anterior cervical surgeries incurred lower costs than posterior surgeries, which incurred lower costs than anterior-posterior surgeries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


