{"title":"Impact of preoperative nutritional impairment on physical function early after total hip arthroplasty.","authors":"Tsutomu Fujita, Satoshi Hamai, Toshimi Konishi, Kazuya Okazawa, Yuki Nasu, Daisuke Hara, Shinya Kawahara, Ryosuke Yamaguchi, Taishi Sato, Ken Utsunomiya, Goro Motomura, Kenichi Kawaguchi, Yasuharu Nakashima","doi":"10.1302/2633-1462.66.BJO-2024-0261.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To investigate whether preoperative nutritional status, assessed by the Geriatric Nutritional Risk Index (GNRI), predicts postoperative physical function following total hip arthroplasty (THA).</p><p><strong>Methods: </strong>A total of 681 patients (87 males, 594 females; mean age 65.3 years (SD 10.2)) who underwent unilateral primary THA for hip osteoarthritis were included. GNRI was calculated from preoperative serum albumin levels, categorizing patients into three groups: normal nutrition (GNRI ≥ 98), moderate malnutrition (92 ≤ GNRI < 98), and severe malnutrition (GNRI < 92). Physical function, including hip joint range of motion, muscle strength (hip abduction, knee extension), leg length difference, and comfortable walking speed, was assessed preoperatively and at discharge. Group comparisons were made based on GNRI scores, and a multiple regression analysis was conducted using preoperative muscle strength ratio and postoperative comfortable walking speed as outcome variables. Receiver operating characteristic curves determined a preoperative GNRI cut-off value for achieving a postoperative comfortable walking speed of 0.8 m/s.</p><p><strong>Results: </strong>The moderate and severe malnutrition comprised 68 (10%) and 19 (3%) patients with GNRI: 92 ≤ GNRI < 98 and < 92, respectively, whereas 594 (87%) were in the normal nutrition (GNRI ≥ 98). Patients with malnutrition demonstrated significantly lower preoperative muscle strength and pre- and postoperative muscle strength ratios (p < 0.001). Preoperative GNRI was a significant predictor of hip abductor muscle strength (p = 0.031) and postoperative comfortable walking speed (p < 0.001). The determined preoperative GNRI cut-off score for achieving a postoperative comfortable walking speed of 0.8 m/s was 98.</p><p><strong>Conclusion: </strong>Preoperative GNRI serves as a valuable indicator for improving postoperative muscle strength and comfortable walking speed.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 6","pages":"667-676"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12145927/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.66.BJO-2024-0261.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: To investigate whether preoperative nutritional status, assessed by the Geriatric Nutritional Risk Index (GNRI), predicts postoperative physical function following total hip arthroplasty (THA).
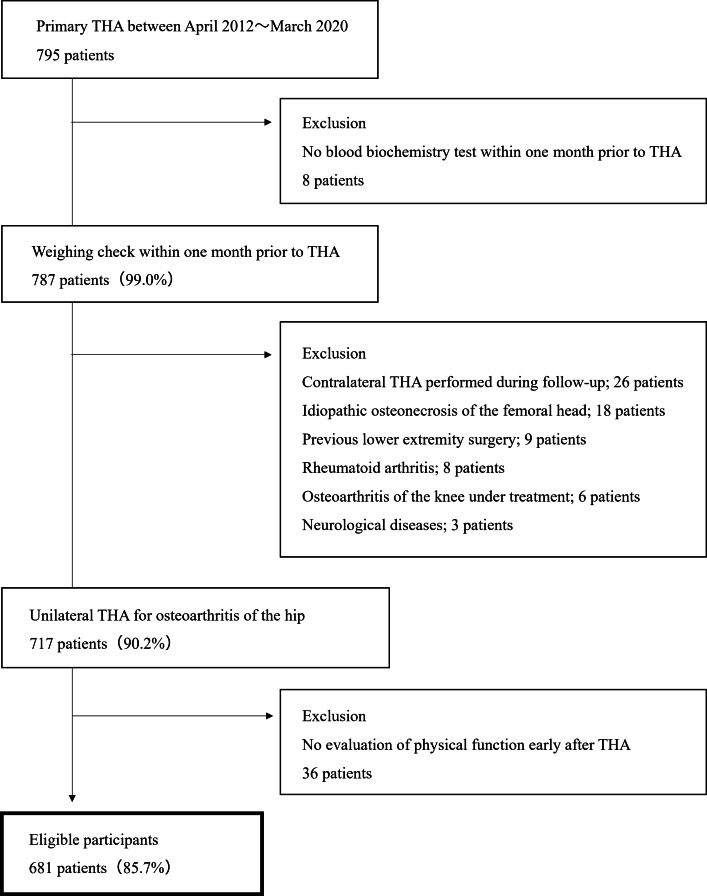
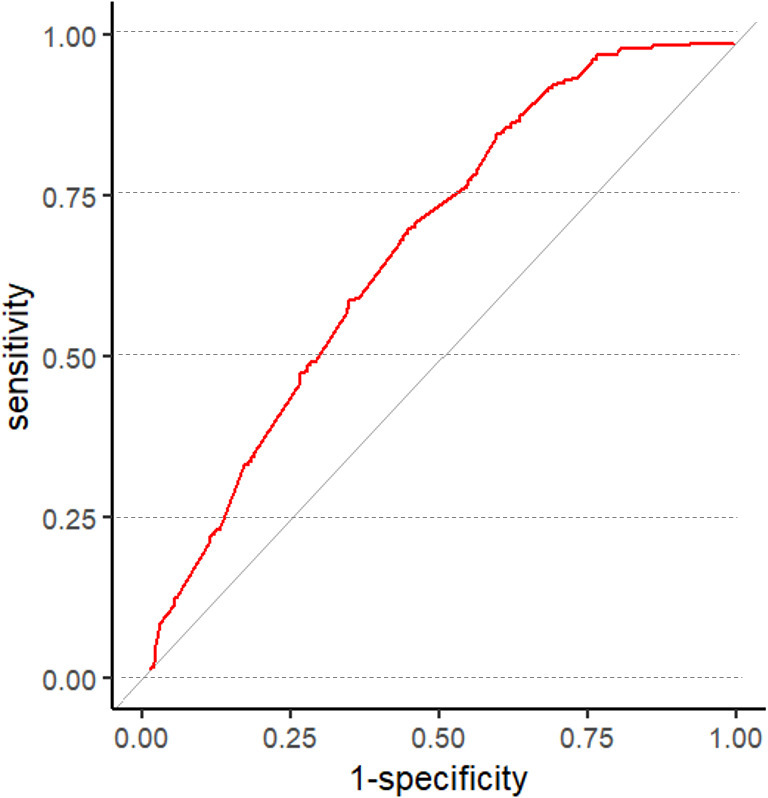
Methods: A total of 681 patients (87 males, 594 females; mean age 65.3 years (SD 10.2)) who underwent unilateral primary THA for hip osteoarthritis were included. GNRI was calculated from preoperative serum albumin levels, categorizing patients into three groups: normal nutrition (GNRI ≥ 98), moderate malnutrition (92 ≤ GNRI < 98), and severe malnutrition (GNRI < 92). Physical function, including hip joint range of motion, muscle strength (hip abduction, knee extension), leg length difference, and comfortable walking speed, was assessed preoperatively and at discharge. Group comparisons were made based on GNRI scores, and a multiple regression analysis was conducted using preoperative muscle strength ratio and postoperative comfortable walking speed as outcome variables. Receiver operating characteristic curves determined a preoperative GNRI cut-off value for achieving a postoperative comfortable walking speed of 0.8 m/s.
Results: The moderate and severe malnutrition comprised 68 (10%) and 19 (3%) patients with GNRI: 92 ≤ GNRI < 98 and < 92, respectively, whereas 594 (87%) were in the normal nutrition (GNRI ≥ 98). Patients with malnutrition demonstrated significantly lower preoperative muscle strength and pre- and postoperative muscle strength ratios (p < 0.001). Preoperative GNRI was a significant predictor of hip abductor muscle strength (p = 0.031) and postoperative comfortable walking speed (p < 0.001). The determined preoperative GNRI cut-off score for achieving a postoperative comfortable walking speed of 0.8 m/s was 98.
Conclusion: Preoperative GNRI serves as a valuable indicator for improving postoperative muscle strength and comfortable walking speed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


