Maci Clark, Hannah Zerr, Ben Ose, David Fritz, Caroline Trupp, Amulya Gupta, Ahmed Shahab, Amit Noheria, Seth H Sheldon
{"title":"Learning Curve for Left Bundle Branch Area Pacing Lead Implantation.","authors":"Maci Clark, Hannah Zerr, Ben Ose, David Fritz, Caroline Trupp, Amulya Gupta, Ahmed Shahab, Amit Noheria, Seth H Sheldon","doi":"10.19102/icrm.2025.16055","DOIUrl":null,"url":null,"abstract":"<p><p>Left bundle branch area pacing (LBBAP) has shown promising outcomes at experienced centers; however, less is known about the learning curve with initial adoption of LBBAP implantation. We conducted a retrospective analysis (2020-2023) of the learning curve for LBBAP at an academic medical center. Procedural success and device-related adverse events in adult patients undergoing LBBAP by seven new operators with >5 years' experience in device implantation were compared between operators with a history of ≤10 (LBBAP<sub>inexp</sub>) versus >10 (LBBAP<sub>exp</sub>) LBBAP implant attempts. Successful LBBAP was defined as a left ventricular activation time (LVAT) of ≤80 ms. Seven operators implanted LBBAP devices in 288 patients (age, 73 ± 11 years; 38% women), including 68 (24%) in the LBBAP<sub>inexp</sub> group versus 220 (76%) patients in the LBBAP<sub>exp</sub> group with similar baseline characteristics. The median number of implants per operator was 22 (range, 8-83). Post-implant LVAT ≤ 80 ms was less frequent in LBBAP<sub>inexp</sub> compared to LBBAP<sub>exp</sub> (56.9% vs 72.4%; <i>P</i> = .04). There were no significant differences in paced QRS duration ≤ 130 ms (75.9% vs. 76.1%; <i>P</i> = 1.0) or operator self-identified success (85% vs. 91%; <i>P</i> = .2). With new single-/dual-chamber device implants, there was no difference in implant duration (103.4 ± 31.8 vs. 101.6 ± 38.5 min; <i>P</i> = .3), but there was longer fluoroscopy with LBBAP<sub>inexp</sub> (12.6 ± 10.1 vs. 8.2 ± 8.0 min; <i>P</i> < .0001). The average number of attempts at LBBAP was lower with LBBAP<sub>inexp</sub> versus LBBAP<sub>exp</sub> (2.0 ± 1.5 vs. 2.9 ± 2.9; <i>P</i> = .03). There was no difference in device-related adverse events between the two groups (<i>P</i> = .3). Operators use less fluoroscopy, make more attempts at LBBAP, and more frequently achieve LVAT ≤ 80 ms after their first 10 implants.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"16 5","pages":"6284-6291"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12140124/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2025.16055","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
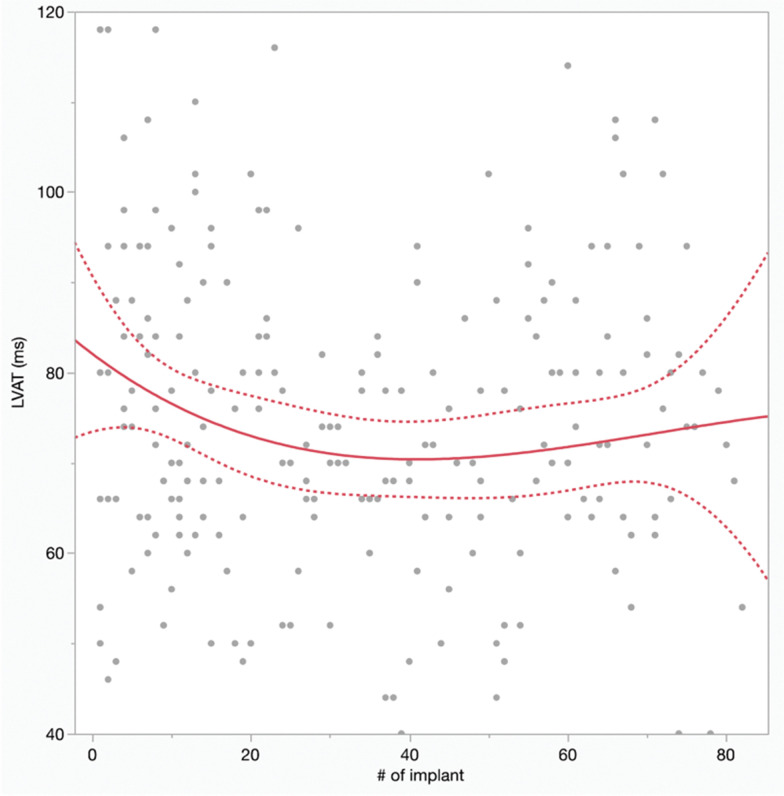
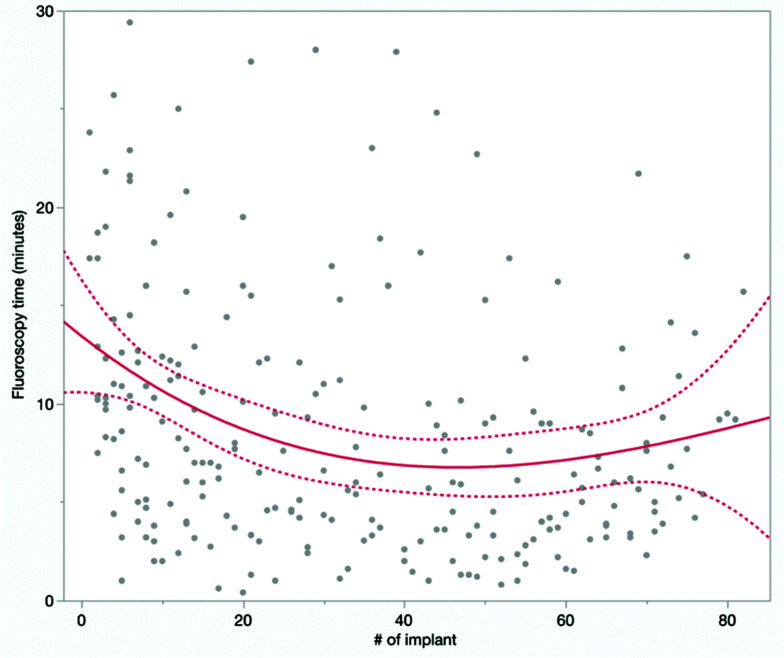
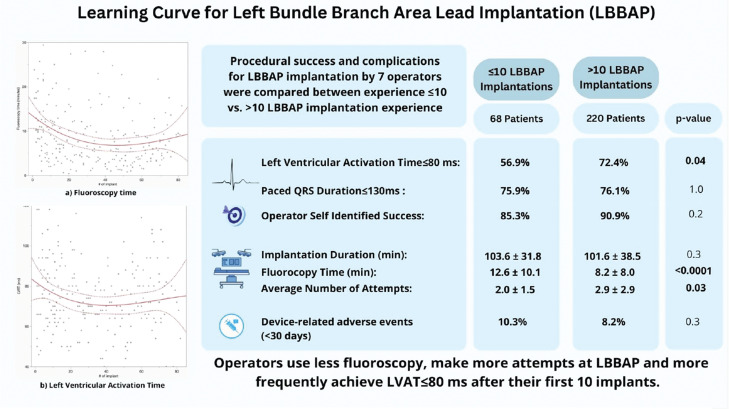
Left bundle branch area pacing (LBBAP) has shown promising outcomes at experienced centers; however, less is known about the learning curve with initial adoption of LBBAP implantation. We conducted a retrospective analysis (2020-2023) of the learning curve for LBBAP at an academic medical center. Procedural success and device-related adverse events in adult patients undergoing LBBAP by seven new operators with >5 years' experience in device implantation were compared between operators with a history of ≤10 (LBBAPinexp) versus >10 (LBBAPexp) LBBAP implant attempts. Successful LBBAP was defined as a left ventricular activation time (LVAT) of ≤80 ms. Seven operators implanted LBBAP devices in 288 patients (age, 73 ± 11 years; 38% women), including 68 (24%) in the LBBAPinexp group versus 220 (76%) patients in the LBBAPexp group with similar baseline characteristics. The median number of implants per operator was 22 (range, 8-83). Post-implant LVAT ≤ 80 ms was less frequent in LBBAPinexp compared to LBBAPexp (56.9% vs 72.4%; P = .04). There were no significant differences in paced QRS duration ≤ 130 ms (75.9% vs. 76.1%; P = 1.0) or operator self-identified success (85% vs. 91%; P = .2). With new single-/dual-chamber device implants, there was no difference in implant duration (103.4 ± 31.8 vs. 101.6 ± 38.5 min; P = .3), but there was longer fluoroscopy with LBBAPinexp (12.6 ± 10.1 vs. 8.2 ± 8.0 min; P < .0001). The average number of attempts at LBBAP was lower with LBBAPinexp versus LBBAPexp (2.0 ± 1.5 vs. 2.9 ± 2.9; P = .03). There was no difference in device-related adverse events between the two groups (P = .3). Operators use less fluoroscopy, make more attempts at LBBAP, and more frequently achieve LVAT ≤ 80 ms after their first 10 implants.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


