{"title":"Assessing Upfront Treatment Patterns for Newly Initiated Patients With Pulmonary Arterial Hypertension in the United States.","authors":"Carly Paoli, Wenze Tang, Sumeet Panjabi, Ashwin Ravichandran","doi":"10.36469/001c.138006","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) pulmonary hypertension guidelines recommend initial combination of endothelin receptor antagonist (ERA) and phosphodiesterase type-5 inhibitor (PDE5i) in patients with pulmonary arterial hypertension (PAH) at low to intermediate risk without cardiopulmonary comorbidities. <b>Objective:</b> To examine US treatment patterns for newly diagnosed patients, including frequency of cardiopulmonary comorbidities. <b>Methods:</b> Treatment-naïve adults (≥18 years) initiating treatment, identified using claims data (IQVIA PharMetrics® Plus; April 2013-June 2023), were assigned dual therapy if initiating ERA/PDE5i within a treatment-determination period (3 months), or monotherapy if initiating ERA or PDE5i. Descriptive statistics captured 25th/75th percentiles, means (SD), and medians. <b>Results:</b> Of 2868 patients, 824 (28.7%) initiated dual therapy and 2044 (71.3%) monotherapy. In dual therapy, 461 (56.0%) initiated ERA first, 250 (30.3%) PDE5i first, and 113 (13.7%) both the same day. In monotherapy, 153 (7.5%) received ERA and 1891 (92.5%) PDE5i. For escalation to dual therapy, 330 (16.1%) monotherapy users initiated ERA (10.7%) or PDE5i (5.5%) during follow-up. Most had cardiopulmonary comorbidities (monotherapy: 86.8%; dual: 79.6%). Of the 824 on dual therapy, 20.4% started triple therapy during follow-up. Compared with monotherapy, dual therapy users were younger (54.9 vs 59.6 years) and mostly female (72.9% vs 60.9%). <b>Discussion:</b> This study found that in the United States, among newly diagnosed PAH patients, 71.3% initiated monotherapy and 28.7% dual therapy, with 16.1% of monotherapy patients eventually escalating to dual therapy. High rates of initial monotherapy may reflect the high proportion of patients with comorbidities and their possible intolerance of initial dual therapy. As these data mostly precede the 2022 guidelines, future research should include treatment post-guidelines, rationales behind decision making, differences between initial monotherapy and dual therapy users, and monotherapy overreliance and effects on morbidity and mortality. <b>Conclusions:</b> This analysis of real-world US treatment patterns for newly initiating PAH patients found low rates of upfront dual-therapy use with high rates of cardiopulmonary comorbidities.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 1","pages":"213-221"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12145179/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.138006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
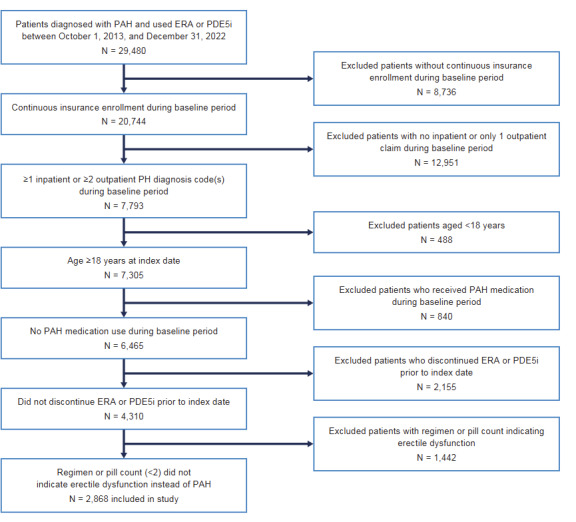
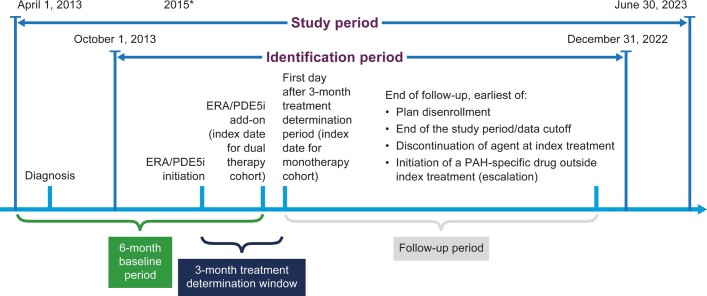
Background: The 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) pulmonary hypertension guidelines recommend initial combination of endothelin receptor antagonist (ERA) and phosphodiesterase type-5 inhibitor (PDE5i) in patients with pulmonary arterial hypertension (PAH) at low to intermediate risk without cardiopulmonary comorbidities. Objective: To examine US treatment patterns for newly diagnosed patients, including frequency of cardiopulmonary comorbidities. Methods: Treatment-naïve adults (≥18 years) initiating treatment, identified using claims data (IQVIA PharMetrics® Plus; April 2013-June 2023), were assigned dual therapy if initiating ERA/PDE5i within a treatment-determination period (3 months), or monotherapy if initiating ERA or PDE5i. Descriptive statistics captured 25th/75th percentiles, means (SD), and medians. Results: Of 2868 patients, 824 (28.7%) initiated dual therapy and 2044 (71.3%) monotherapy. In dual therapy, 461 (56.0%) initiated ERA first, 250 (30.3%) PDE5i first, and 113 (13.7%) both the same day. In monotherapy, 153 (7.5%) received ERA and 1891 (92.5%) PDE5i. For escalation to dual therapy, 330 (16.1%) monotherapy users initiated ERA (10.7%) or PDE5i (5.5%) during follow-up. Most had cardiopulmonary comorbidities (monotherapy: 86.8%; dual: 79.6%). Of the 824 on dual therapy, 20.4% started triple therapy during follow-up. Compared with monotherapy, dual therapy users were younger (54.9 vs 59.6 years) and mostly female (72.9% vs 60.9%). Discussion: This study found that in the United States, among newly diagnosed PAH patients, 71.3% initiated monotherapy and 28.7% dual therapy, with 16.1% of monotherapy patients eventually escalating to dual therapy. High rates of initial monotherapy may reflect the high proportion of patients with comorbidities and their possible intolerance of initial dual therapy. As these data mostly precede the 2022 guidelines, future research should include treatment post-guidelines, rationales behind decision making, differences between initial monotherapy and dual therapy users, and monotherapy overreliance and effects on morbidity and mortality. Conclusions: This analysis of real-world US treatment patterns for newly initiating PAH patients found low rates of upfront dual-therapy use with high rates of cardiopulmonary comorbidities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


