Katherine M Tang, Cloyde Mills, Teresa A McCann, Susan L Rosenthal, Jennifer Lee
{"title":"Using Quality Improvement Methods to Reduce Length of Stay with a Respiratory Therapist-driven Pathway for Asthma.","authors":"Katherine M Tang, Cloyde Mills, Teresa A McCann, Susan L Rosenthal, Jennifer Lee","doi":"10.1097/pq9.0000000000000817","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Asthma pathways reduce hospital length of stay (LOS), and respiratory therapists (RTs) can optimize care. This study aimed to use quality improvement methods to implement an asthma-specific RT role and RT-driven asthma pathway. The SMART aim was to reduce LOS for pediatric patients admitted for asthma to the general inpatient units by 20% within 22 months.</p><p><strong>Methods: </strong>We included children 2-17 years of age who were admitted to a general inpatient unit for asthma. We excluded patients transferred from another hospital, initially admitted to the pediatric intensive care unit, or with comorbidities predisposed to severe respiratory illnesses. We used the Model for Improvement to design and study interventions. Key drivers focused on standardizing care, leveraging provider expertise, and supporting providers with education and technology. The outcome measure was LOS. The main process measure was the early transition to an albuterol metered-dose inhaler. Balancing measures were hospital reutilization rates and escalation of care. We used statistical process control charts and run charts to analyze the data.</p><p><strong>Results: </strong>The study included 743 patients, with 339 in the intervention period. The intervention group had a younger median age (4 [3, 7] versus 6 [3, 10] years, <i>P</i> < 0.001) and more publicly insured patients (84% versus 68%, <i>P</i> < 0.001). LOS decreased from 39.4 to 30.7 hours, achieving our SMART aim without adversely affecting the balancing measures.</p><p><strong>Conclusions: </strong>Quality improvement methodology aids in implementing an RT-driven asthma pathway on the pediatric floors to decrease LOS without adversely influencing hospital reutilization rates or transfers for escalation of care.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 3","pages":"e817"},"PeriodicalIF":1.1000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12140678/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000817","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
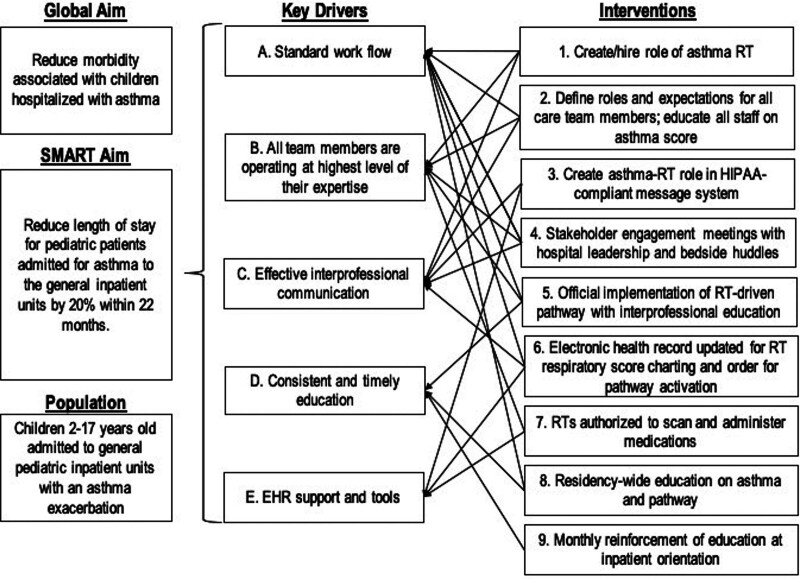
Introduction: Asthma pathways reduce hospital length of stay (LOS), and respiratory therapists (RTs) can optimize care. This study aimed to use quality improvement methods to implement an asthma-specific RT role and RT-driven asthma pathway. The SMART aim was to reduce LOS for pediatric patients admitted for asthma to the general inpatient units by 20% within 22 months.
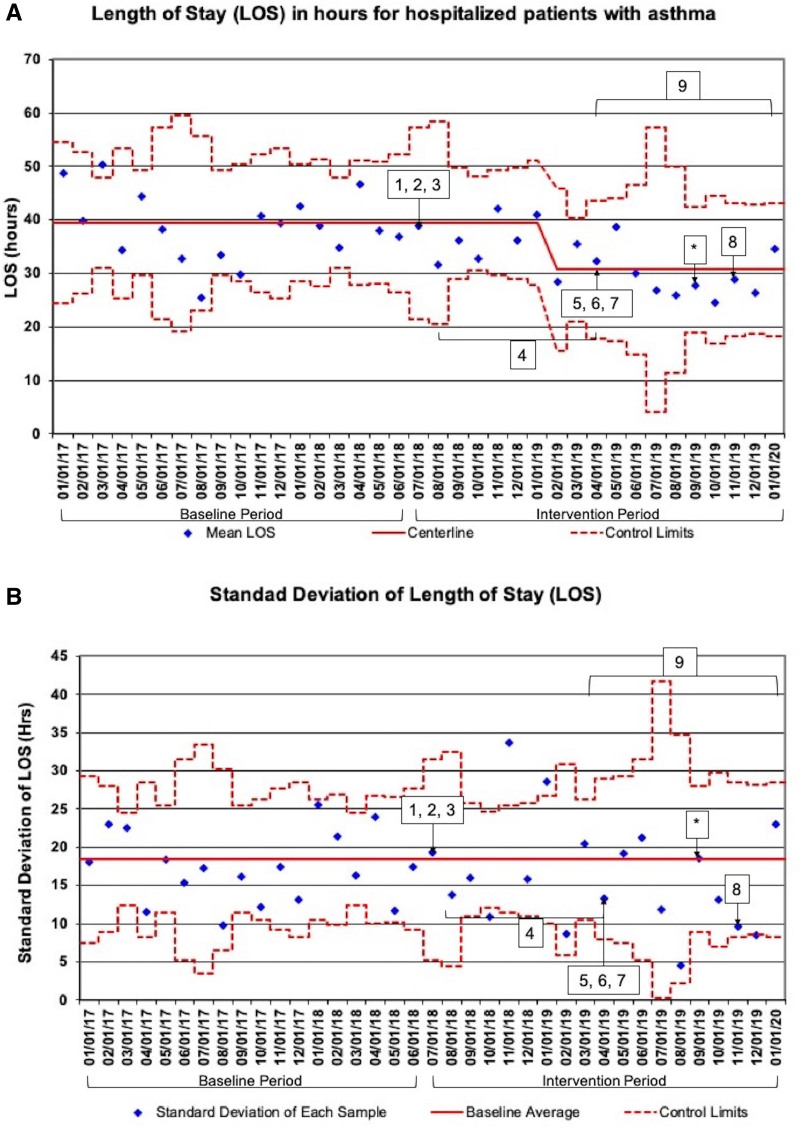
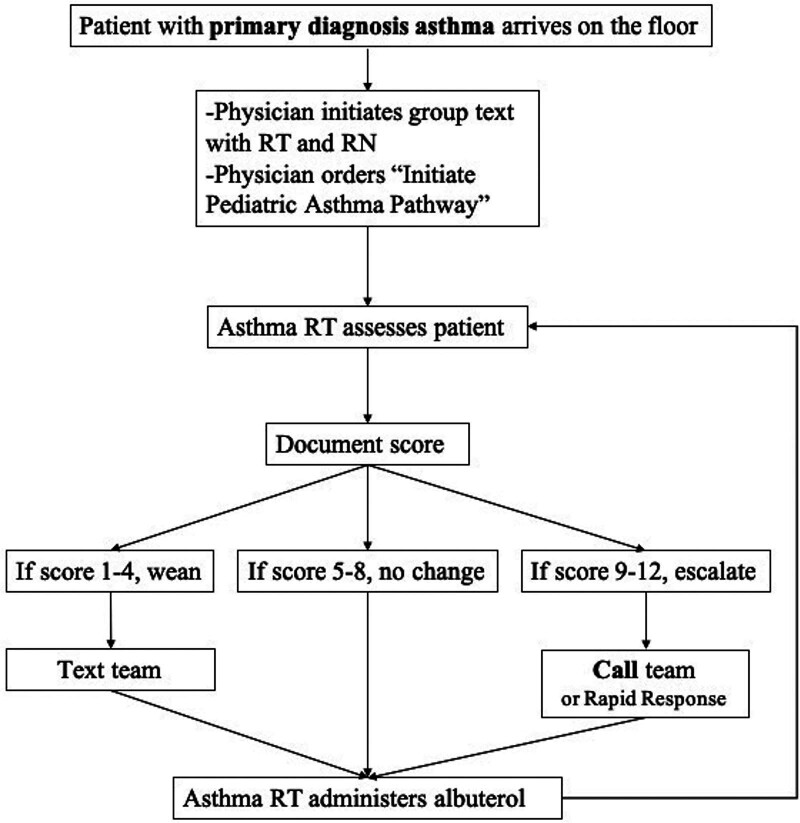
Methods: We included children 2-17 years of age who were admitted to a general inpatient unit for asthma. We excluded patients transferred from another hospital, initially admitted to the pediatric intensive care unit, or with comorbidities predisposed to severe respiratory illnesses. We used the Model for Improvement to design and study interventions. Key drivers focused on standardizing care, leveraging provider expertise, and supporting providers with education and technology. The outcome measure was LOS. The main process measure was the early transition to an albuterol metered-dose inhaler. Balancing measures were hospital reutilization rates and escalation of care. We used statistical process control charts and run charts to analyze the data.
Results: The study included 743 patients, with 339 in the intervention period. The intervention group had a younger median age (4 [3, 7] versus 6 [3, 10] years, P < 0.001) and more publicly insured patients (84% versus 68%, P < 0.001). LOS decreased from 39.4 to 30.7 hours, achieving our SMART aim without adversely affecting the balancing measures.
Conclusions: Quality improvement methodology aids in implementing an RT-driven asthma pathway on the pediatric floors to decrease LOS without adversely influencing hospital reutilization rates or transfers for escalation of care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


