Mark R J Jenkinson, Calvin Cheung, Alastair G Dick, Johan Witt, Jonathan Hutt
{"title":"Functional pelvic tilt frequently differs from the anterior pelvic plane in non-arthritic hip disorders : implications for 3D motion analysis.","authors":"Mark R J Jenkinson, Calvin Cheung, Alastair G Dick, Johan Witt, Jonathan Hutt","doi":"10.1302/2633-1462.66.BJO-2024-0265.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Hip preservation surgeons are increasingly using commercially available 3D motion analysis software to investigate areas of impingement and quantify femoral head coverage. Variations in functional pelvic tilt will affect the position of the acetabular rim and projected femoral head coverage, but currently the majority of available software standardizes sagittal rotation to the anterior pelvic plane (APP). The study hypothesis was that the APP does not correlate well with patient-specific pelvic position.</p><p><strong>Methods: </strong>In total, 60 patients were selected from an institutional database: 20 with acetabular retroversion (AR), 20 with developmental dysplasia of the hip (DDH), and 20 with cam-type femoroacetabular impingement (FAI). Multiplanar CT reformats were created and the sagittal rotation was aligned to the APP. The sagittal pelvic orientation was then corrected until the anteroposterior (AP) projection mirrored that of their preoperative supine and standing plain radiographs. The change in sagittal pelvic tilt angle required was measured.</p><p><strong>Results: </strong>The mean deviation from the APP in the AR group was 11.55° (SD 4.96°) for supine radiographs and 3.28° (SD 8.66°) for standing radiographs. The mean deviation from the APP in the DDH group was 12.2° (SD 4.26°) for supine radiographs and 6.96° (SD 3.43°) for standing radiographs. The main deviation from the APP in the FAI group was 8.63° (SD 5.21°) for supine radiographs and -1.28° (SD 7.31°) for standing.</p><p><strong>Conclusion: </strong>There is a wide variation in patients' functional pelvic positioning in both supine and standing radiographs, in all different subgroups, which rarely correlates with the APP. Commercial 3D motion analysis may therefore give misleading results for both the extent and location of hip impingement as well as femoral head coverage, which may affect surgical decision-making. Consideration should be given to incorporating this into the software algorithms.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 6","pages":"651-657"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12140813/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.66.BJO-2024-0265.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Hip preservation surgeons are increasingly using commercially available 3D motion analysis software to investigate areas of impingement and quantify femoral head coverage. Variations in functional pelvic tilt will affect the position of the acetabular rim and projected femoral head coverage, but currently the majority of available software standardizes sagittal rotation to the anterior pelvic plane (APP). The study hypothesis was that the APP does not correlate well with patient-specific pelvic position.
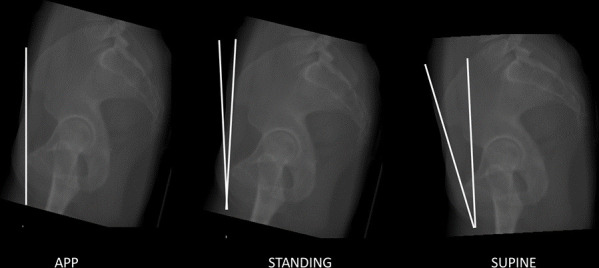
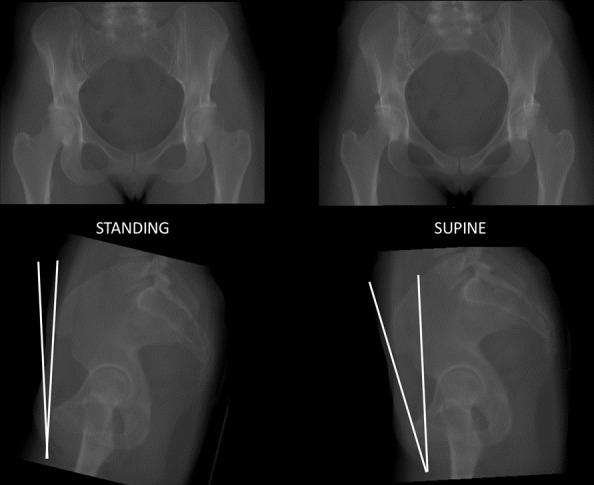
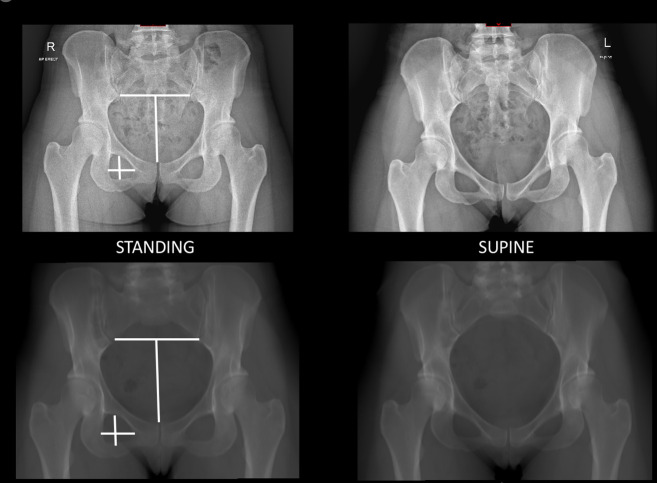
Methods: In total, 60 patients were selected from an institutional database: 20 with acetabular retroversion (AR), 20 with developmental dysplasia of the hip (DDH), and 20 with cam-type femoroacetabular impingement (FAI). Multiplanar CT reformats were created and the sagittal rotation was aligned to the APP. The sagittal pelvic orientation was then corrected until the anteroposterior (AP) projection mirrored that of their preoperative supine and standing plain radiographs. The change in sagittal pelvic tilt angle required was measured.
Results: The mean deviation from the APP in the AR group was 11.55° (SD 4.96°) for supine radiographs and 3.28° (SD 8.66°) for standing radiographs. The mean deviation from the APP in the DDH group was 12.2° (SD 4.26°) for supine radiographs and 6.96° (SD 3.43°) for standing radiographs. The main deviation from the APP in the FAI group was 8.63° (SD 5.21°) for supine radiographs and -1.28° (SD 7.31°) for standing.
Conclusion: There is a wide variation in patients' functional pelvic positioning in both supine and standing radiographs, in all different subgroups, which rarely correlates with the APP. Commercial 3D motion analysis may therefore give misleading results for both the extent and location of hip impingement as well as femoral head coverage, which may affect surgical decision-making. Consideration should be given to incorporating this into the software algorithms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


