Abdulraouf M Z Jijeh, Ghassan A Shaath, Sameh R Ismail, Mohamed S Kabbani, Omar M Hijazi, Hayan Altaweel, Husam Hamada, Ammar Qadi, Anis Fatima, Abdrabo Abdrabo, Wiaam Ahmed, Nuha Ahmed, Ahmed Elsaoudi, Ahmed Yousef, Rehana Shafi, Husam I Ardah, Ahmad Elwy, Abdullah A Alghamdi
{"title":"Optimizing Recovery: Early Versus Delayed Chest Tube Removal in Pediatric Cardiac Surgery Patients: A Randomized Controlled Trial.","authors":"Abdulraouf M Z Jijeh, Ghassan A Shaath, Sameh R Ismail, Mohamed S Kabbani, Omar M Hijazi, Hayan Altaweel, Husam Hamada, Ammar Qadi, Anis Fatima, Abdrabo Abdrabo, Wiaam Ahmed, Nuha Ahmed, Ahmed Elsaoudi, Ahmed Yousef, Rehana Shafi, Husam I Ardah, Ahmad Elwy, Abdullah A Alghamdi","doi":"10.1097/CCE.0000000000001271","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the safety and efficacy of an early chest tube removal protocol in reducing tube duration without increasing complications following pediatric cardiac surgery.</p><p><strong>Design: </strong>A single-center, randomized controlled trial.</p><p><strong>Setting: </strong>Pediatric cardiac ICU.</p><p><strong>Patients: </strong>Two hundred fifteen pediatric patients with chest tubes after cardiac surgery.</p><p><strong>Interventions: </strong>Patients were randomized to early removal (drainage threshold < 6 mL/kg over 8 hr) or late removal (24-hr assessment) groups. Primary outcomes included chest tube duration, whereas secondary outcomes encompassed ICU stay, ventilation time, hospital stay, and complication rates.</p><p><strong>Measurements and main results: </strong>Median chest tube duration was significantly shorter in the early removal group (3 d) compared with the late removal group (4.9 d; p < 0.0001). Rates of fluid reaccumulation and pneumothorax were low and comparable between groups. Notably, no patients in either group required tube reinsertion. ICU and total hospital stay durations were similar across groups.</p><p><strong>Conclusions: </strong>An early chest tube removal protocol following pediatric cardiac surgery suggests a reduction in chest tube duration without increasing the risk of complications. These findings support the adoption of an evidence-based early removal approach to enhance patient comfort and optimize ICU resource utilization in pediatric cardiac surgery patients.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 6","pages":"e1271"},"PeriodicalIF":2.7000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12140733/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001271","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the safety and efficacy of an early chest tube removal protocol in reducing tube duration without increasing complications following pediatric cardiac surgery.
Design: A single-center, randomized controlled trial.
Setting: Pediatric cardiac ICU.
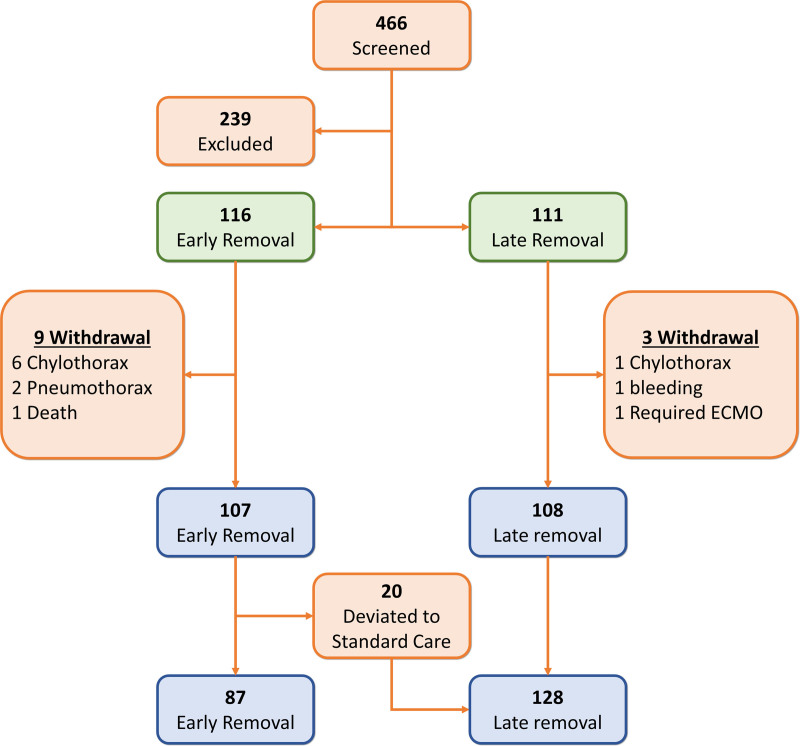
Patients: Two hundred fifteen pediatric patients with chest tubes after cardiac surgery.
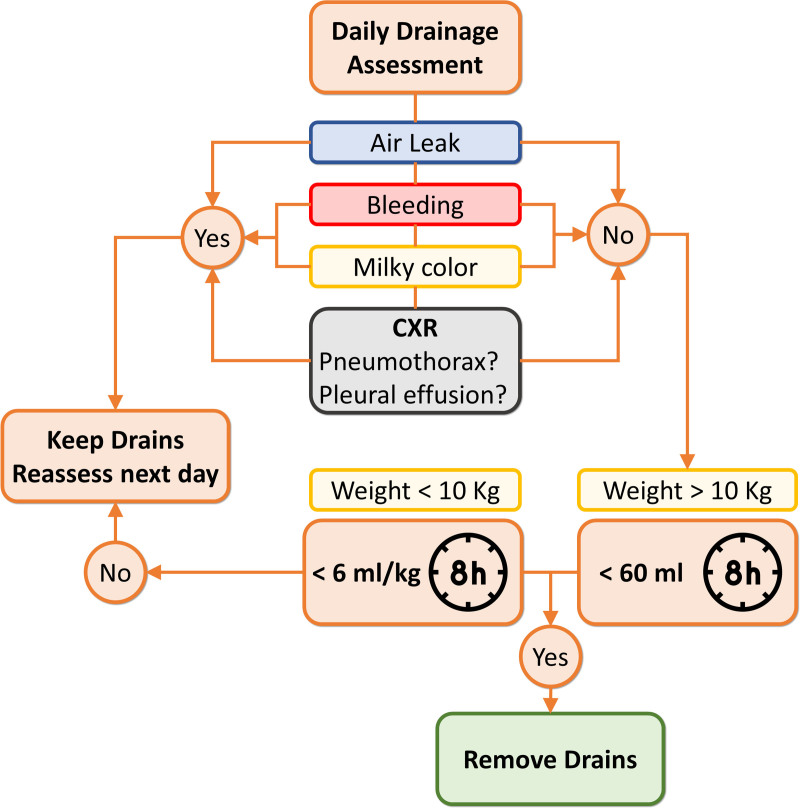
Interventions: Patients were randomized to early removal (drainage threshold < 6 mL/kg over 8 hr) or late removal (24-hr assessment) groups. Primary outcomes included chest tube duration, whereas secondary outcomes encompassed ICU stay, ventilation time, hospital stay, and complication rates.
Measurements and main results: Median chest tube duration was significantly shorter in the early removal group (3 d) compared with the late removal group (4.9 d; p < 0.0001). Rates of fluid reaccumulation and pneumothorax were low and comparable between groups. Notably, no patients in either group required tube reinsertion. ICU and total hospital stay durations were similar across groups.
Conclusions: An early chest tube removal protocol following pediatric cardiac surgery suggests a reduction in chest tube duration without increasing the risk of complications. These findings support the adoption of an evidence-based early removal approach to enhance patient comfort and optimize ICU resource utilization in pediatric cardiac surgery patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


