Amelia F Wong, Jaime K Otillio, Abby K Fahnestock, Christine M Smith, Michael R DeBaun, Emmanuel Volanakis, Lacey Noffsinger, Jeannie Byrd, S Barron Frazier
{"title":"Reducing Time to Analgesia for Sickle Cell Pain Episode Treatment in the Pediatric Emergency Department.","authors":"Amelia F Wong, Jaime K Otillio, Abby K Fahnestock, Christine M Smith, Michael R DeBaun, Emmanuel Volanakis, Lacey Noffsinger, Jeannie Byrd, S Barron Frazier","doi":"10.1097/pq9.0000000000000821","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pain episodes are the most common emergency department (ED) presentation for patients with sickle cell disease (SCD). Prompt pain medication and frequent pain assessments are recommended. Our SMART aim was to reduce the time from ED rooming to first analgesia administration for children presenting with SCD pain from 50 to less than 30 minutes by June 2024.</p><p><strong>Methods: </strong>Children presenting to the ED with a diagnosis of SCD requiring opioids for pain were included. The primary outcome was time from rooming to analgesia. A key driver diagram, developed by a multidisciplinary team, informed our interventions and then implemented through plan-do-study-act cycles. Statistical process control charts were used to analyze data with Nelson rules to detect special cause variation. Secondary measures included frequency of pain assessments in the first 2 hours and ED length of stay.</p><p><strong>Results: </strong>From July 2020 to June 2024, there were 447 eligible encounters. Baseline data (n = 143) revealed an average time from ED rooming to analgesia of 50 minutes. Following interventions, including order set implementation, multidisciplinary collaboration, and incorporating the home action plan in the ED, special cause variation was detected with a centerline shift to 32 minutes. The median number of pain assessments in the first 2 hours of arrival improved from 2.2 to 2.7 with order set utilization. ED length of stay remained unchanged.</p><p><strong>Conclusions: </strong>Standardizing care with an order set increased the number of pain assessments. Incorporation of the SCD home pain action plan into the ED treatment pathway decreased the time to analgesia.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 3","pages":"e821"},"PeriodicalIF":1.1000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136660/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000821","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Pain episodes are the most common emergency department (ED) presentation for patients with sickle cell disease (SCD). Prompt pain medication and frequent pain assessments are recommended. Our SMART aim was to reduce the time from ED rooming to first analgesia administration for children presenting with SCD pain from 50 to less than 30 minutes by June 2024.
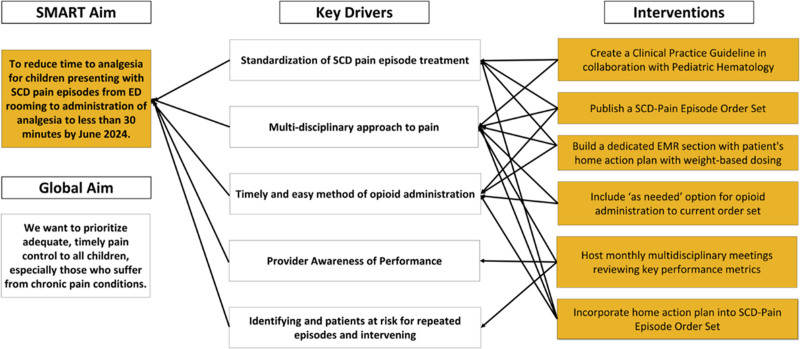
Methods: Children presenting to the ED with a diagnosis of SCD requiring opioids for pain were included. The primary outcome was time from rooming to analgesia. A key driver diagram, developed by a multidisciplinary team, informed our interventions and then implemented through plan-do-study-act cycles. Statistical process control charts were used to analyze data with Nelson rules to detect special cause variation. Secondary measures included frequency of pain assessments in the first 2 hours and ED length of stay.
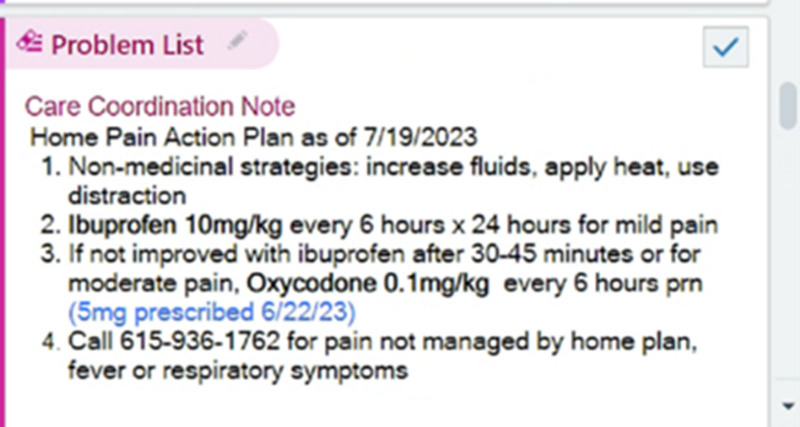
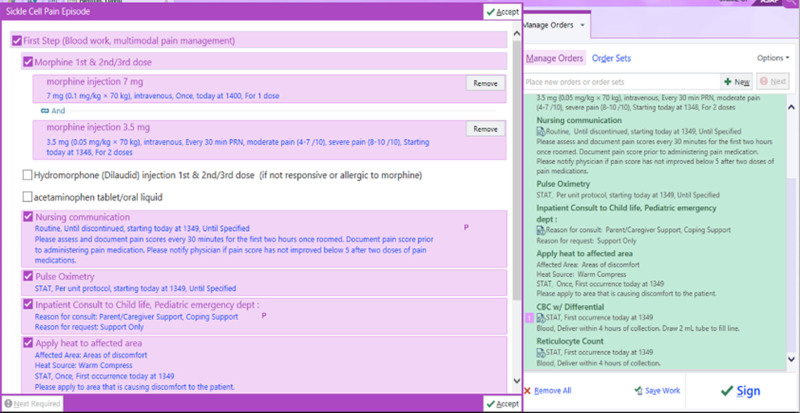
Results: From July 2020 to June 2024, there were 447 eligible encounters. Baseline data (n = 143) revealed an average time from ED rooming to analgesia of 50 minutes. Following interventions, including order set implementation, multidisciplinary collaboration, and incorporating the home action plan in the ED, special cause variation was detected with a centerline shift to 32 minutes. The median number of pain assessments in the first 2 hours of arrival improved from 2.2 to 2.7 with order set utilization. ED length of stay remained unchanged.
Conclusions: Standardizing care with an order set increased the number of pain assessments. Incorporation of the SCD home pain action plan into the ED treatment pathway decreased the time to analgesia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


