A nomogram integrating clinical stage and pre-EBV DNA to identify the cycles of induction chemotherapy for locoregionally advanced nasopharyngeal carcinoma.
{"title":"A nomogram integrating clinical stage and pre-EBV DNA to identify the cycles of induction chemotherapy for locoregionally advanced nasopharyngeal carcinoma.","authors":"Sunqin Cai, Zongwei Huang, Zihan Chen, Ying Li, Jingjing Su, Ronghui Chen, Siqi Xu, Jing Wang, Sufang Qiu","doi":"10.1186/s13014-025-02672-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This research focused on determining the optimal cycles of induction chemotherapy (IC) in high-risk locoregionally advanced nasopharyngeal carcinoma (LA-NPC).</p><p><strong>Methods: </strong>The retrospective analysis was conducted on 885 patients. Potential bias was minimized by propensity score matching (PSM). Overall survival (OS) served as the primary endpoint. Survival outcomes were analyzed using Kaplan-Meier curves, with statistical comparisons performed via the log-rank test. Prognostic determinants were identified through multivariate cox regression analysis. A nomogram model was constructed to quantify individualized prognosis.</p><p><strong>Results: </strong>Patients were divided into 2/3-cycle (IC = 2/3) and 4-cycle IC (IC = 4) groups. After PSM, 446 patients remained and were categorized into distinct risk groups according to independent predictors, including clinical stage and pre-treatment Epstein-Barr virus DNA (pre-EBV DNA). For the high-risk cohort (stage IVa with pre-EBV DNA ≥ 4000 copies/mL), the IC = 4 regimen showed higher 5-year OS (70.4% vs. 54.7%, P = 0.036) than the IC = 2/3 regimen. In the low- and middle-risk cohorts, the IC = 2/3 regimen exhibited OS comparable to the IC = 4 regimen. The established nomogram model demonstrated superior prognostic power compared to individual factors. Given the adverse effects, the IC = 4 regimen was associated with significantly higher rates of grade 3-4 neutropenia (24.6% vs. 15.5%, P = 0.017) and thrombocytopenia (8.0% vs. 3.7%, P = 0.049) compared to the IC = 2/3 regimen.</p><p><strong>Conclusion: </strong>The developed nomogram offers personalized guidance on selecting individual IC cycles for LA-NPC patients.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"93"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12139057/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02672-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This research focused on determining the optimal cycles of induction chemotherapy (IC) in high-risk locoregionally advanced nasopharyngeal carcinoma (LA-NPC).
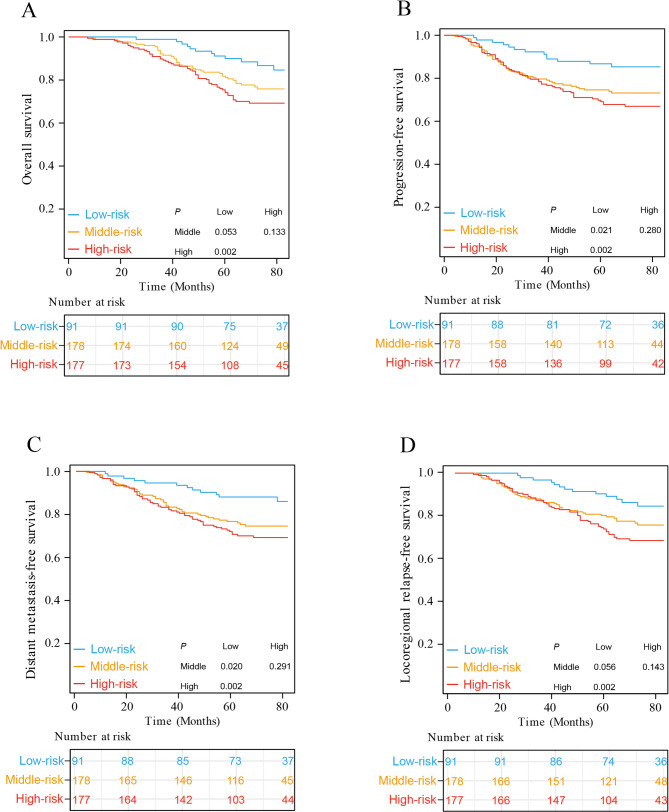
Methods: The retrospective analysis was conducted on 885 patients. Potential bias was minimized by propensity score matching (PSM). Overall survival (OS) served as the primary endpoint. Survival outcomes were analyzed using Kaplan-Meier curves, with statistical comparisons performed via the log-rank test. Prognostic determinants were identified through multivariate cox regression analysis. A nomogram model was constructed to quantify individualized prognosis.
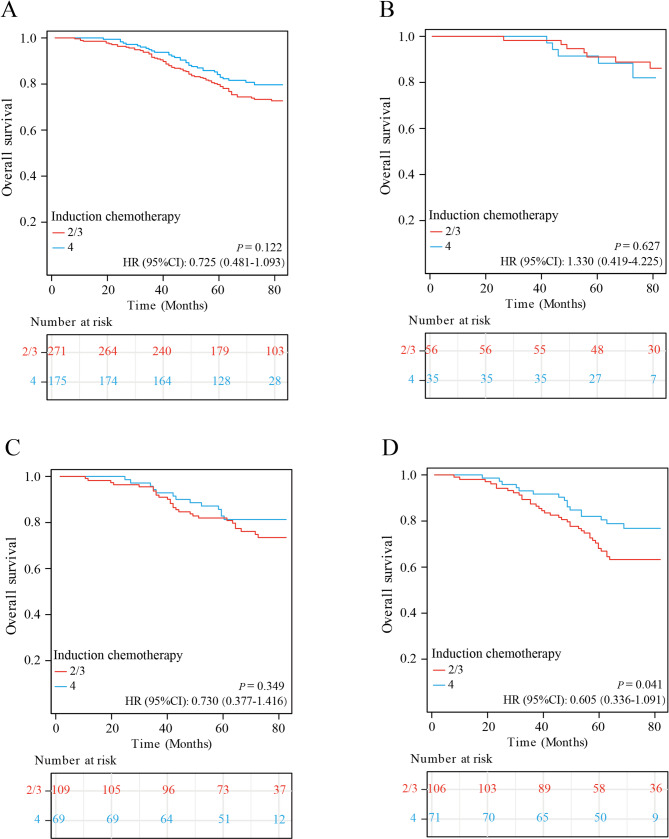
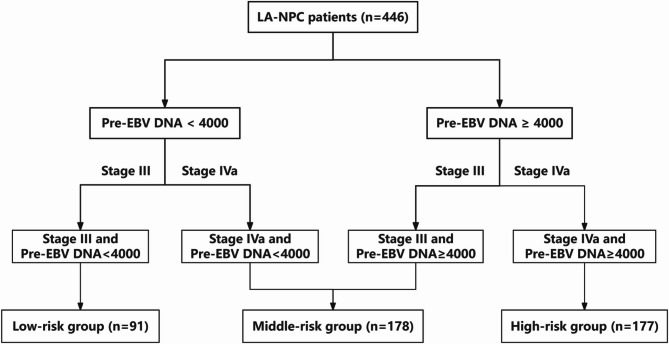
Results: Patients were divided into 2/3-cycle (IC = 2/3) and 4-cycle IC (IC = 4) groups. After PSM, 446 patients remained and were categorized into distinct risk groups according to independent predictors, including clinical stage and pre-treatment Epstein-Barr virus DNA (pre-EBV DNA). For the high-risk cohort (stage IVa with pre-EBV DNA ≥ 4000 copies/mL), the IC = 4 regimen showed higher 5-year OS (70.4% vs. 54.7%, P = 0.036) than the IC = 2/3 regimen. In the low- and middle-risk cohorts, the IC = 2/3 regimen exhibited OS comparable to the IC = 4 regimen. The established nomogram model demonstrated superior prognostic power compared to individual factors. Given the adverse effects, the IC = 4 regimen was associated with significantly higher rates of grade 3-4 neutropenia (24.6% vs. 15.5%, P = 0.017) and thrombocytopenia (8.0% vs. 3.7%, P = 0.049) compared to the IC = 2/3 regimen.
Conclusion: The developed nomogram offers personalized guidance on selecting individual IC cycles for LA-NPC patients.
目的:探讨局部晚期鼻咽癌(LA-NPC)高危患者诱导化疗(IC)的最佳周期。方法:对885例患者进行回顾性分析。通过倾向评分匹配(PSM)最小化潜在偏倚。总生存期(OS)作为主要终点。生存结果采用Kaplan-Meier曲线进行分析,通过log-rank检验进行统计学比较。通过多变量cox回归分析确定预后决定因素。建立nomogram模型来量化个体化预后。结果:患者分为2/3周期组(IC = 2/3)和4周期组(IC = 4)。PSM后,446例患者保留,并根据独立预测因子,包括临床分期和治疗前eb病毒DNA (pre-EBV DNA),分为不同的风险组。对于高危队列(IVa期,ebv前DNA≥4000拷贝/mL), IC = 4方案的5年OS高于IC = 2/3方案(70.4% vs. 54.7%, P = 0.036)。在低风险和中风险队列中,IC = 2/3方案的OS与IC = 4方案相当。与个体因素相比,所建立的nomogram模型显示出更强的预后能力。考虑到不良反应,与IC = 2/3方案相比,IC = 4方案与3-4级中性粒细胞减少症(24.6% vs 15.5%, P = 0.017)和血小板减少症(8.0% vs 3.7%, P = 0.049)的发生率显著升高。结论:开发的nomogram脑电图为LA-NPC患者的IC周期选择提供了个性化的指导。
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


