Alexia Le Corre, Adel Maamar, Mathieu Lederlin, Nicolas Terzi, Jean-Marc Tadié, Arnaud Gacouin
{"title":"Are presentations of thoracic CT performed on admission to the ICU associated with mortality at day-90 in COVID-19 related ARDS?","authors":"Alexia Le Corre, Adel Maamar, Mathieu Lederlin, Nicolas Terzi, Jean-Marc Tadié, Arnaud Gacouin","doi":"10.1186/s41479-025-00166-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Computed tomography (CT) analysis of lung morphology has significantly advanced our understanding of acute respiratory distress syndrome (ARDS). During the Coronavirus Disease 2019 (COVID-19) pandemic, CT imaging was widely utilized to evaluate lung injury and was suggested as a tool for predicting patient outcomes. However, data specifically focused on patients with ARDS admitted to intensive care units (ICUs) remain limited.</p><p><strong>Methods: </strong>This retrospective study analyzed patients admitted to ICUs between March 2020 and November 2022 with moderate to severe COVID-19 ARDS. All CT scans performed within 48 h of ICU admission were independently reviewed by three experts. Lung injury severity was quantified using the CT Severity Score (CT-SS; range 0-25). Patients were categorized as having severe disease (CT-SS ≥ 18) or non-severe disease (CT-SS < 18). The primary outcome was all-cause mortality at 90 days. Secondary outcomes included ICU mortality and medical complications during the ICU stay. Additionally, we evaluated a computer-assisted CT-score assessment using artificial intelligence software (CT Pneumonia Analysis<sup>®</sup>, SIEMENS Healthcare) to explore the feasibility of automated measurement and routine implementation.</p><p><strong>Results: </strong>A total of 215 patients with moderate to severe COVID-19 ARDS were included. The median CT-SS at admission was 18/25 [interquartile range, 15-21]. Among them, 120 patients (56%) had a severe CT-SS (≥ 18), while 95 patients (44%) had a non-severe CT-SS (< 18). The 90-day mortality rates were 20.8% for the severe group and 15.8% for the non-severe group (p = 0.35). No significant association was observed between CT-SS severity and patient outcomes.</p><p><strong>Conclusion: </strong>In patients with moderate to severe COVID-19 ARDS, systematic CT assessment of lung parenchymal injury was not a reliable predictor of 90-day mortality or ICU-related complications.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"17 1","pages":"14"},"PeriodicalIF":6.2000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12139360/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-025-00166-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Computed tomography (CT) analysis of lung morphology has significantly advanced our understanding of acute respiratory distress syndrome (ARDS). During the Coronavirus Disease 2019 (COVID-19) pandemic, CT imaging was widely utilized to evaluate lung injury and was suggested as a tool for predicting patient outcomes. However, data specifically focused on patients with ARDS admitted to intensive care units (ICUs) remain limited.
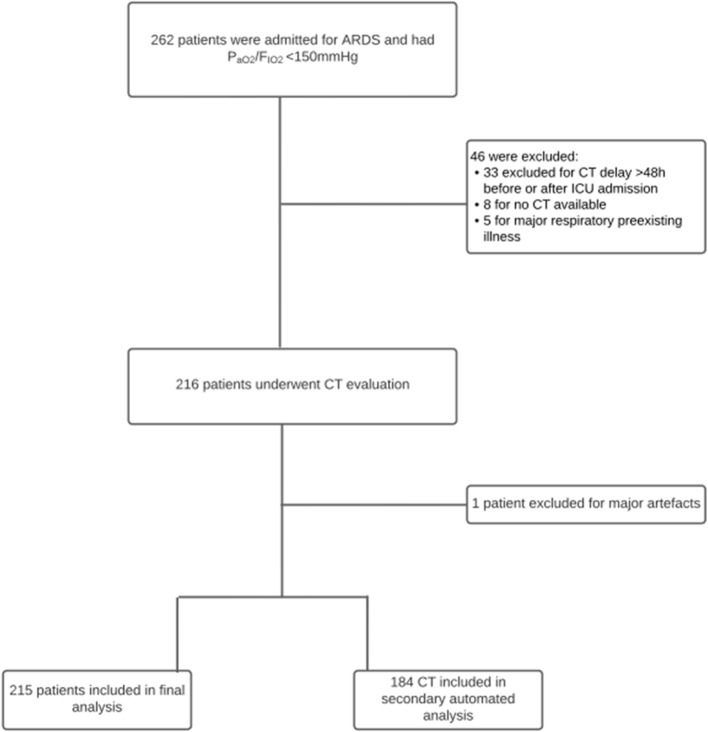
Methods: This retrospective study analyzed patients admitted to ICUs between March 2020 and November 2022 with moderate to severe COVID-19 ARDS. All CT scans performed within 48 h of ICU admission were independently reviewed by three experts. Lung injury severity was quantified using the CT Severity Score (CT-SS; range 0-25). Patients were categorized as having severe disease (CT-SS ≥ 18) or non-severe disease (CT-SS < 18). The primary outcome was all-cause mortality at 90 days. Secondary outcomes included ICU mortality and medical complications during the ICU stay. Additionally, we evaluated a computer-assisted CT-score assessment using artificial intelligence software (CT Pneumonia Analysis®, SIEMENS Healthcare) to explore the feasibility of automated measurement and routine implementation.
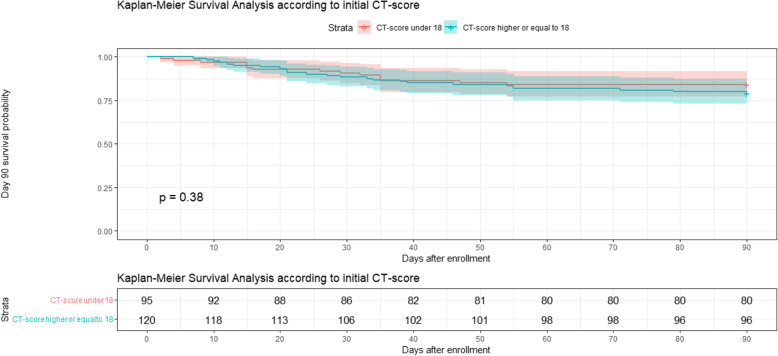
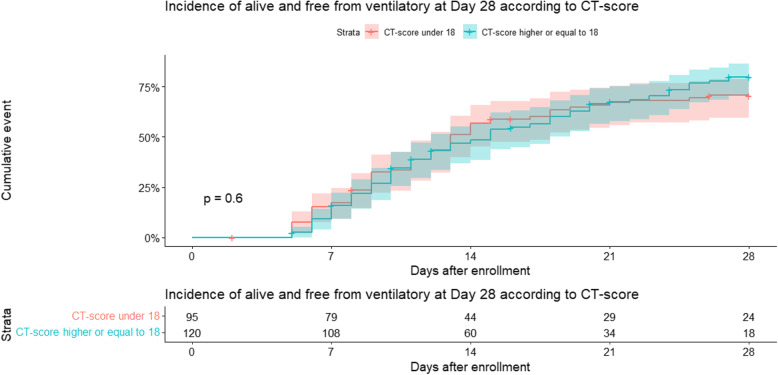
Results: A total of 215 patients with moderate to severe COVID-19 ARDS were included. The median CT-SS at admission was 18/25 [interquartile range, 15-21]. Among them, 120 patients (56%) had a severe CT-SS (≥ 18), while 95 patients (44%) had a non-severe CT-SS (< 18). The 90-day mortality rates were 20.8% for the severe group and 15.8% for the non-severe group (p = 0.35). No significant association was observed between CT-SS severity and patient outcomes.
Conclusion: In patients with moderate to severe COVID-19 ARDS, systematic CT assessment of lung parenchymal injury was not a reliable predictor of 90-day mortality or ICU-related complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


