Michele E Haumann, Adrie Bekker, Chandre Geldenhuys, Natasha O'Connell, Andrew Whitelaw, Tonya Esterhuizen, Angela Dramowski
{"title":"Prevalence of carbapenem-resistant Enterobacterales colonisation in hospitalised neonates.","authors":"Michele E Haumann, Adrie Bekker, Chandre Geldenhuys, Natasha O'Connell, Andrew Whitelaw, Tonya Esterhuizen, Angela Dramowski","doi":"10.4102/sajid.v40i1.726","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Carbapenem-resistant Enterobacterales (CRE) have emerged as major healthcare-associated infection (HAI) pathogens globally with substantial associated mortality and morbidity.</p><p><strong>Objectives: </strong>We conducted a retrospective cohort study to determine the prevalence of rectal CRE colonisation in neonates referred from a central hospital, to a regional and a district hospital in the Western Cape Province of South Africa (01 March 2019 - 30 September 2020).</p><p><strong>Method: </strong>Clinical data and laboratory records were reviewed to identify possible factors associated with CRE colonisation using stepwise forward logistic regression analysis.</p><p><strong>Results: </strong>Among 291 neonates transferred to the regional and district hospitals, the median birth weight and gestational age were 1360 (interquartile range [IQR]: 1080 g - 1690 g) and 31 (IQR: 29-33) weeks. The overall CRE rectal colonisation prevalence at the time of transfer from the central hospital was 22.3% (65/291), with colonising species including <i>Klebsiella pneumoniae</i> (59/65, 90.8%) and <i>Serratia marcescens</i> (6/65; 9.2%). There were no factors significantly associated with CRE colonisation. No CRE-colonised neonate subsequently developed CRE infection. Post-discharge mortality rates were similar in the CRE-colonised versus the non-colonised neonates (2/65 [3.1%] vs. 9/226 [4.0%]; <i>p</i> = 0.737).</p><p><strong>Conclusion: </strong>There was no increased risk of subsequent CRE infection or mortality in the 12 months post-discharge in neonates who were CRE colonised.</p><p><strong>Contribution: </strong>Rectal colonisation with CRE was highly prevalent in preterm neonates being transferred for step-down hospital care. Carbapenem-resistant Enterobacterales-colonised neonates had similar demographic characteristics to non-colonised neonates, with no factors significantly associated with CRE colonisation.</p>","PeriodicalId":44007,"journal":{"name":"Southern African Journal of Infectious Diseases","volume":"40 1","pages":"726"},"PeriodicalIF":1.3000,"publicationDate":"2025-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12135765/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Southern African Journal of Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/sajid.v40i1.726","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Carbapenem-resistant Enterobacterales (CRE) have emerged as major healthcare-associated infection (HAI) pathogens globally with substantial associated mortality and morbidity.
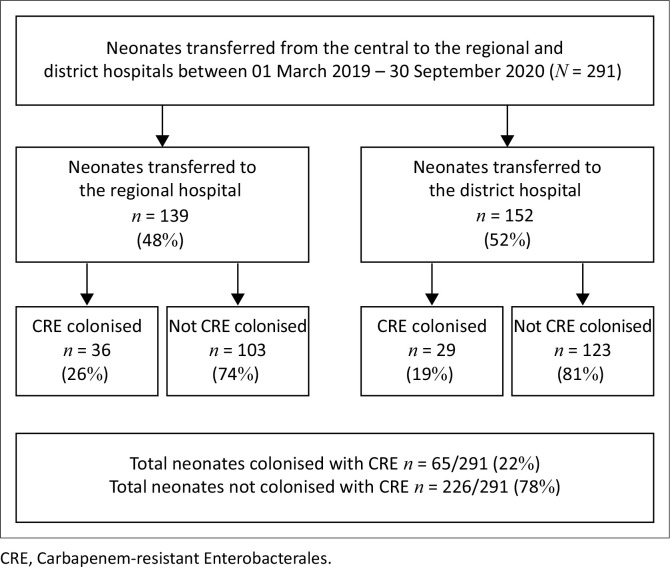
Objectives: We conducted a retrospective cohort study to determine the prevalence of rectal CRE colonisation in neonates referred from a central hospital, to a regional and a district hospital in the Western Cape Province of South Africa (01 March 2019 - 30 September 2020).
Method: Clinical data and laboratory records were reviewed to identify possible factors associated with CRE colonisation using stepwise forward logistic regression analysis.
Results: Among 291 neonates transferred to the regional and district hospitals, the median birth weight and gestational age were 1360 (interquartile range [IQR]: 1080 g - 1690 g) and 31 (IQR: 29-33) weeks. The overall CRE rectal colonisation prevalence at the time of transfer from the central hospital was 22.3% (65/291), with colonising species including Klebsiella pneumoniae (59/65, 90.8%) and Serratia marcescens (6/65; 9.2%). There were no factors significantly associated with CRE colonisation. No CRE-colonised neonate subsequently developed CRE infection. Post-discharge mortality rates were similar in the CRE-colonised versus the non-colonised neonates (2/65 [3.1%] vs. 9/226 [4.0%]; p = 0.737).
Conclusion: There was no increased risk of subsequent CRE infection or mortality in the 12 months post-discharge in neonates who were CRE colonised.
Contribution: Rectal colonisation with CRE was highly prevalent in preterm neonates being transferred for step-down hospital care. Carbapenem-resistant Enterobacterales-colonised neonates had similar demographic characteristics to non-colonised neonates, with no factors significantly associated with CRE colonisation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


