Feasibility, safety and efficiency of an over-pressure wash-in method using fresh gas flow 0.5 L and sevoflurane 8% during initiation of low-flow anaesthesia: A randomised, descriptional study.
Bandi Joshiraj, Harihar V Hegde, Sriramamoorthy R Marimuthu, Manisha Paul, Neethu George
{"title":"Feasibility, safety and efficiency of an over-pressure wash-in method using fresh gas flow 0.5 L and sevoflurane 8% during initiation of low-flow anaesthesia: A randomised, descriptional study.","authors":"Bandi Joshiraj, Harihar V Hegde, Sriramamoorthy R Marimuthu, Manisha Paul, Neethu George","doi":"10.4103/ija.ija_83_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Low-flow anaesthesia (LFA) typically involves a high fresh gas flow (FGF) of 4-6 L/min during the wash-in phase. We aimed to assess the feasibility, safety, and efficiency of an over-pressure wash-in method (FGF = 0.5 L and sevoflurane = 8%) of LFA. The primary objective was the time required to achieve a fraction of alveolar sevoflurane (FAS) =2% (target). Secondary objectives included breathing system stability, ephedrine use, and gas consumption.</p><p><strong>Methods: </strong>After obtaining ethical clearance and consent, 48 patients aged 18-65 years were randomised to two groups: 'conventional' (Group C) and 'over-pressure' (Group OP). During the wash-in phase, FGF was set at 6 L/min with a sevoflurane vaporiser dial (FVS) of 3% in Group C and at 0.5 L/min with an FVS of 8% in Group OP. After achieving a FAS of 2%, FGF was reduced to 0.5 L/min in Group C, and FVS was adjusted to 4% in both groups, which were maintained for 15 min. The unpaired <i>t</i>-test was used to compare quantitative, normally distributed data, while the Mann-Whitney U test was used to compare quantitative, discrete data. A <i>P</i> value of less than 0.05 was considered statistically significant.</p><p><strong>Results: </strong>Data from 45 patients (23 in Group C and 22 in Group OP) were analysed. The mean T<sub>target</sub> was significantly less in Group C than in Group OP [314 (SD: 145) vs 478 (SD: 100) s, <i>P</i> < 0.001]. The breathing system was 'stable' in a significantly higher number of patients (number, percentage) in Group OP compared to Group C (19, 86.4% vs 8, 34.8%) (<i>P</i> = 0.001). The number of vaporiser dial adjustments was significantly different (<i>P</i> = 0.005). The mean consumption of oxygen [50.7 (SD: 6.6) vs 36.4 (SD: 1.2) L, <i>P</i> < 0.001], air [19.2 (SD: 6.8) vs 4.0 (SD: 0.3) L, <i>P</i> < 0.001], and sevoflurane [6.7 (SD: 2) vs 3.3 (SD: 1) mL, <i>P</i> < 0.001] was significantly higher in Group C compared to Group OP.</p><p><strong>Conclusion: </strong>Our method of over-pressure wash-in during LFA initiation is simple, feasible, safe, efficient, economical, and environmentally friendly.</p>","PeriodicalId":13339,"journal":{"name":"Indian Journal of Anaesthesia","volume":"69 6","pages":"580-586"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12133035/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ija.ija_83_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
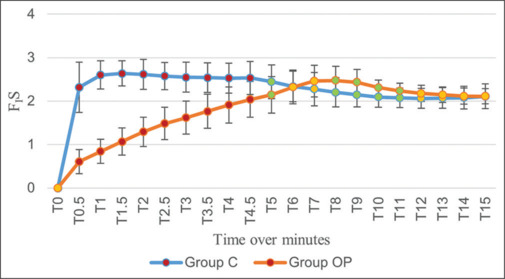
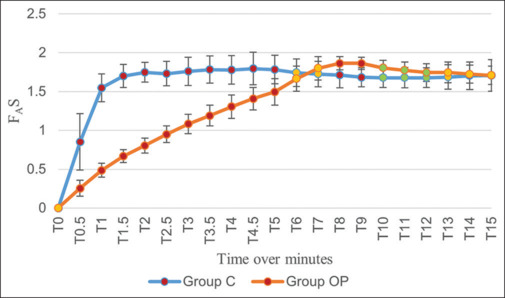
Background and aims: Low-flow anaesthesia (LFA) typically involves a high fresh gas flow (FGF) of 4-6 L/min during the wash-in phase. We aimed to assess the feasibility, safety, and efficiency of an over-pressure wash-in method (FGF = 0.5 L and sevoflurane = 8%) of LFA. The primary objective was the time required to achieve a fraction of alveolar sevoflurane (FAS) =2% (target). Secondary objectives included breathing system stability, ephedrine use, and gas consumption.
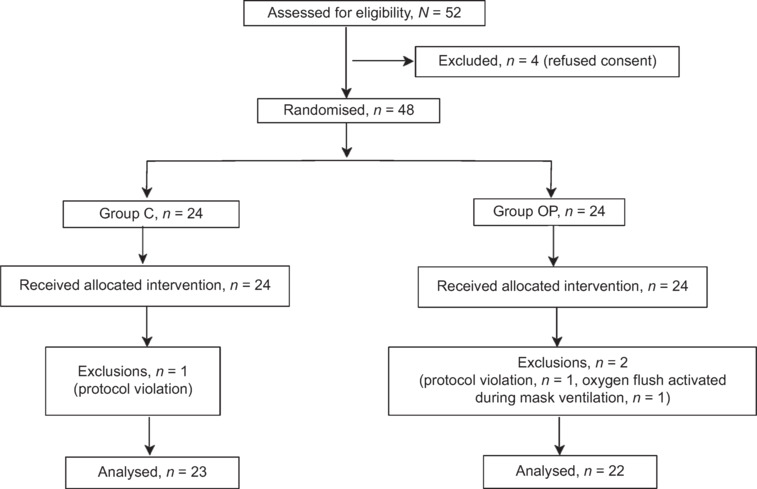
Methods: After obtaining ethical clearance and consent, 48 patients aged 18-65 years were randomised to two groups: 'conventional' (Group C) and 'over-pressure' (Group OP). During the wash-in phase, FGF was set at 6 L/min with a sevoflurane vaporiser dial (FVS) of 3% in Group C and at 0.5 L/min with an FVS of 8% in Group OP. After achieving a FAS of 2%, FGF was reduced to 0.5 L/min in Group C, and FVS was adjusted to 4% in both groups, which were maintained for 15 min. The unpaired t-test was used to compare quantitative, normally distributed data, while the Mann-Whitney U test was used to compare quantitative, discrete data. A P value of less than 0.05 was considered statistically significant.
Results: Data from 45 patients (23 in Group C and 22 in Group OP) were analysed. The mean Ttarget was significantly less in Group C than in Group OP [314 (SD: 145) vs 478 (SD: 100) s, P < 0.001]. The breathing system was 'stable' in a significantly higher number of patients (number, percentage) in Group OP compared to Group C (19, 86.4% vs 8, 34.8%) (P = 0.001). The number of vaporiser dial adjustments was significantly different (P = 0.005). The mean consumption of oxygen [50.7 (SD: 6.6) vs 36.4 (SD: 1.2) L, P < 0.001], air [19.2 (SD: 6.8) vs 4.0 (SD: 0.3) L, P < 0.001], and sevoflurane [6.7 (SD: 2) vs 3.3 (SD: 1) mL, P < 0.001] was significantly higher in Group C compared to Group OP.
Conclusion: Our method of over-pressure wash-in during LFA initiation is simple, feasible, safe, efficient, economical, and environmentally friendly.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


