{"title":"Prognostic factors after salvage resection for local progression of brain metastases after radiotherapy.","authors":"Hideyuki Arita, Toshiki Ikawa, Naoyuki Kanayama, Masahiro Morimoto, Toru Umehara, Hidenori Yoshizawa, Yoshinori Kodama, Yoshiko Okita, Manabu Kinoshita, Koji Konishi","doi":"10.1007/s00701-025-06578-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recent advances in cancer treatment have prolonged survival after the onset of brain metastasis (BM), increasing the incidence of local progression (LP) following radiotherapy. However, no standard approach exists for managing LP. We aimed to evaluate the outcomes of salvage surgery in a clinical setting.</p><p><strong>Methods: </strong>The clinical data were retrospectively collected from the medical records of 49 patients who underwent their first salvage surgery for LP of BM at a single institution between April 2014 and March 2024. Overall survival (OS) and LP-free survival (LPFS) were evaluated using the Kaplan-Meier method.</p><p><strong>Results: </strong>Most patients (47/49, 96%) had a history of stereotactic radiosurgery (n = 34) and/or stereotactic radiotherapy (n = 14). The histopathological examination of surgical specimens confirmed tumor recurrence in 33 patients and radiation necrosis (RN) in 16 patients. The interval from prior radiotherapy to salvage surgery was longer in patients with RN than in those with recurrence (median: 42.3 vs. 9.3 months, respectively). OS was longer in the RN group compared with the recurrent group (median: 68.5 months and 21.8 months, respectively). In the recurrent group, shorter OS was associated with preoperative poor KPS (< 70), the presence of active extracranial lesions, and RPA classes 2-3. The extent of resection, postoperative chemotherapy, and local irradiation had no significant effect on OS. After salvage surgery, further LP was observed in 20 patients (61%), with a median LPFS of 7.0 months in the recurrent group. No significant association was found between LPFS and the extent of tumor removal, postoperative chemotherapy, and RT.</p><p><strong>Conclusions: </strong>This study highlights a relatively prolonged survival period following salvage surgery for local progression of BM after irradiation. Salvage surgery is a treatment option in patients with good extracranial control and performance status. The high recurrence rate following salvage treatment underscores the need for developing additional treatment approaches.</p>","PeriodicalId":7370,"journal":{"name":"Acta Neurochirurgica","volume":"167 1","pages":"163"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12141103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Neurochirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00701-025-06578-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Recent advances in cancer treatment have prolonged survival after the onset of brain metastasis (BM), increasing the incidence of local progression (LP) following radiotherapy. However, no standard approach exists for managing LP. We aimed to evaluate the outcomes of salvage surgery in a clinical setting.
Methods: The clinical data were retrospectively collected from the medical records of 49 patients who underwent their first salvage surgery for LP of BM at a single institution between April 2014 and March 2024. Overall survival (OS) and LP-free survival (LPFS) were evaluated using the Kaplan-Meier method.
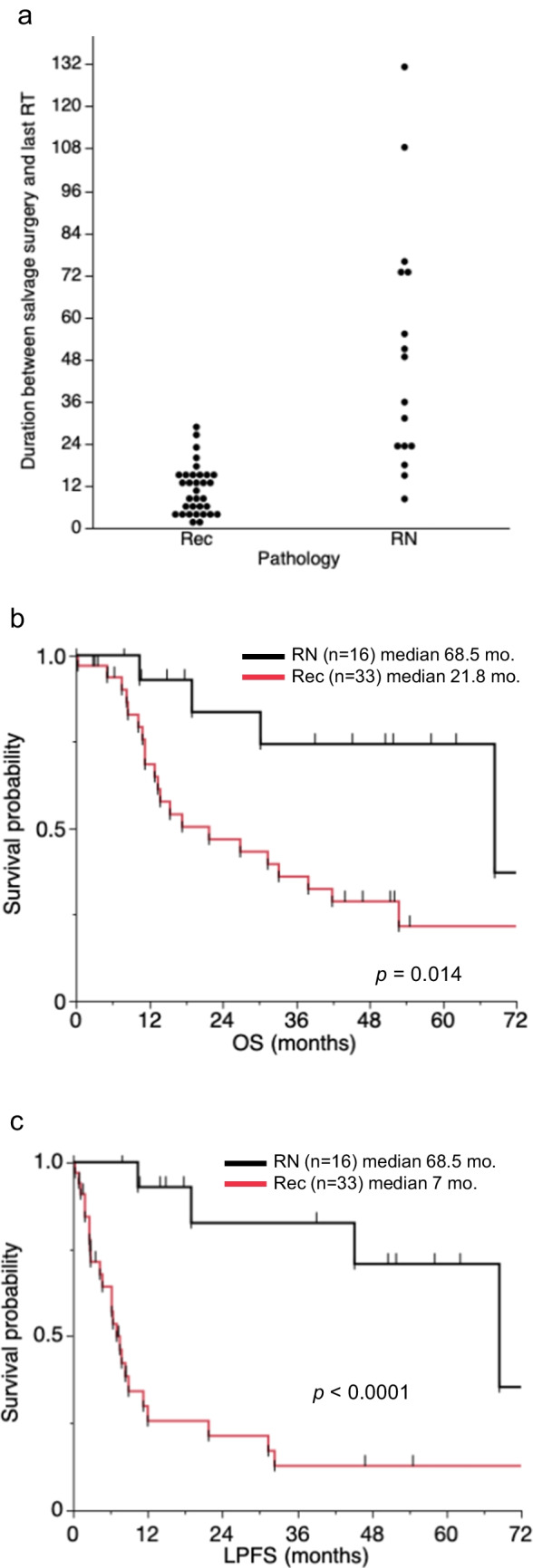
Results: Most patients (47/49, 96%) had a history of stereotactic radiosurgery (n = 34) and/or stereotactic radiotherapy (n = 14). The histopathological examination of surgical specimens confirmed tumor recurrence in 33 patients and radiation necrosis (RN) in 16 patients. The interval from prior radiotherapy to salvage surgery was longer in patients with RN than in those with recurrence (median: 42.3 vs. 9.3 months, respectively). OS was longer in the RN group compared with the recurrent group (median: 68.5 months and 21.8 months, respectively). In the recurrent group, shorter OS was associated with preoperative poor KPS (< 70), the presence of active extracranial lesions, and RPA classes 2-3. The extent of resection, postoperative chemotherapy, and local irradiation had no significant effect on OS. After salvage surgery, further LP was observed in 20 patients (61%), with a median LPFS of 7.0 months in the recurrent group. No significant association was found between LPFS and the extent of tumor removal, postoperative chemotherapy, and RT.
Conclusions: This study highlights a relatively prolonged survival period following salvage surgery for local progression of BM after irradiation. Salvage surgery is a treatment option in patients with good extracranial control and performance status. The high recurrence rate following salvage treatment underscores the need for developing additional treatment approaches.
期刊介绍:
The journal "Acta Neurochirurgica" publishes only original papers useful both to research and clinical work. Papers should deal with clinical neurosurgery - diagnosis and diagnostic techniques, operative surgery and results, postoperative treatment - or with research work in neuroscience if the underlying questions or the results are of neurosurgical interest. Reports on congresses are given in brief accounts. As official organ of the European Association of Neurosurgical Societies the journal publishes all announcements of the E.A.N.S. and reports on the activities of its member societies. Only contributions written in English will be accepted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


