Effect of pubertal induction with combined gonadotropin therapy on testes development and spermatogenesis in males with gonadotropin deficiency: a cohort study.
Sebastian Castro, Kyla Ng Yin, Francesco d'Aniello, Emma C Alexander, Emily Connolly, Claire Hughes, Lee Martin, Rathi Prasad, Helen L Storr, Ruben H Willemsen, Leo Dunkel, Gary Butler, Sasha R Howard
{"title":"Effect of pubertal induction with combined gonadotropin therapy on testes development and spermatogenesis in males with gonadotropin deficiency: a cohort study.","authors":"Sebastian Castro, Kyla Ng Yin, Francesco d'Aniello, Emma C Alexander, Emily Connolly, Claire Hughes, Lee Martin, Rathi Prasad, Helen L Storr, Ruben H Willemsen, Leo Dunkel, Gary Butler, Sasha R Howard","doi":"10.1093/hropen/hoaf026","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Are recombinant FSH (rFSH) and hCG effective therapies for promoting testicular growth and spermatogenesis in male adolescents and young adults with gonadotropin deficiency?</p><p><strong>Summary answer: </strong>Combined gonadotropin therapy is effective in inducing puberty and promoting spermatogenesis in male adolescents and young adults with gonadotropin deficiency and has the potential to improve adult outcomes relating to both fertility and quality of life.</p><p><strong>What is known already: </strong>Deficiency of pituitary gonadotropins (LH and FSH) due to hypogonadotropic hypogonadism (HH) can result in poor testicular development, low testicular volumes, micropenis and cryptorchidism. Inadequate hormonal replacement can lead to long-term issues, including subfertility or infertility, and reduced quality of life. Exogenous testosterone for pubertal induction can elevate serum testosterone concentrations and induce virilization, but it does not promote testicular development nor induce spermatogenesis. Fertility and testes growth remain primary concerns for patients seeking treatment.</p><p><strong>Study design size duration: </strong>We conducted a retrospective observational review of male adolescents and young adults with gonadotropin deficiency and seeking puberty replacement therapy at two large tertiary centre hospitals in London, UK, from 2010 to 2024.</p><p><strong>Participants/materials setting methods: </strong>A total of 35 males, with diagnosis of congenital hypogonadotropic hypogonadism (CHH: n = 23; further subdivided into those with partial [pHH: n = 8] and those with complete gonadotropin deficiency [cHH: n = 15]), acquired HH (AHH: n = 4) or Kallmann syndrome (KS: n = 8), received combined gonadotropin therapy. We assessed testicular growth and semen quality post-treatment.</p><p><strong>Main results and the role of chance: </strong>The majority of patients were referred for pubertal delay, alone or in combination with cryptorchidism, micropenis or microorchidism. Out of 35 patients, 22 (63%) had previously received testosterone, and the median age at gonadotropin treatment initiation was 15.8 years (range: 11.8-22.7). Semen analysis was obtained in 18 out of 19 patients who had received gonadotropin therapy for a median treatment duration of 21.1 months (range: 4.5-66.9) for rFSH and 19.5 months (range: 8.3-61.1) for hCG. The median sperm count on semen analysis was 8.9 × 10<sup>6</sup>/ml (range: 0.0-54.9). Significant increases were noted in testicular volume (median change after therapy: 10.5 ml [95% CI 9.5-13.6], <i>P</i> < 0.0001), testosterone (median increase: 25.7 nmol/l [95% CI 19.8-31.5], <i>P</i> < 0.0001) and inhibin B levels (67.7 pg/ml [95% CI 18.4-86.7], <i>P</i> = 0.0008).</p><p><strong>Limitations reasons for caution: </strong>The relatively low representation of patients with acquired HH in our study emphasizes the need to extrapolate the findings with caution in this specific subgroup of adolescent males with HH. The study is also an observational one, therefore meaning that some outcomes (such as change in inhibin B concentration) were not collected routinely and not reported for all patients. The observational nature of the study design also accounts for the differences in doses and duration observed in gonadotropin therapy.</p><p><strong>Wider implications of the findings: </strong>The treatment of adult male infertility is particularly difficult in severe forms of gonadotropin deficiency, where there has been no testicular stimulation during mini-puberty or puberty. Appropriate hormonal replacement in puberty with combined gonadotropins can induce testicular maturation and spermatogenesis, but data are limited and at present, there is no international consensus on best practice regimens in adolescent and young adult males. Our treatment protocol induced testicular growth and caused increases in serum testosterone and Sertoli cell biomarkers, and spermatogenesis in 15/18 of patients who had completed semen analysis. This indicates the potential to substantially improve the reproductive, physical, and psychological health of patients who have a significant and unmet need for adequate hormonal replacement during puberty. The study described here included patients with diverse forms of HH (congenital, acquired, complete, and partial HH), thereby providing encouraging results across a variety of subjects with impaired puberty facing increased odds of fertility problems in adulthood. Additionally, we observed similar sperm counts between those who received exogenous testosterone treatment prior to gonadotropin therapy and those who began directly on gonadotropins for pubertal induction. This last finding is aligned with previous data and may help to reassure paediatric endocrinologists with limited access to rFSH or hCG that the use of exogenous testosterone to induce androgen-dependent changes in patients seeking treatment for pubertal delay is unlikely to compromise spermatogenic potential, should gonadotropins become available at a later stage.</p><p><strong>Study funding/competing interests: </strong>S.C. was funded by an ESPE Early Career Scientific Development Grant. S.R.H. was funded by the Wellcome Trust (222049/Z/20/Z) and Barts Charity [MGU0552]. K.N.Y. was employed under the NIHR Specialist Foundation Programme. F.d.A. was funded by the student traineeship, University of Rome 'Tor Vergata', an Erasmus Grant and an ESPE Early Career Scientific Development Grant. E.C.A. was funded by an NIHR Academic Clinical Fellowship (ACF-2021-19-002). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care. G.B. received an ESPE Mid-Career Research Fellowship to enable the development of the clinical treatment schedule. The authors have no conflicting interests.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 2","pages":"hoaf026"},"PeriodicalIF":11.1000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12132099/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: Are recombinant FSH (rFSH) and hCG effective therapies for promoting testicular growth and spermatogenesis in male adolescents and young adults with gonadotropin deficiency?
Summary answer: Combined gonadotropin therapy is effective in inducing puberty and promoting spermatogenesis in male adolescents and young adults with gonadotropin deficiency and has the potential to improve adult outcomes relating to both fertility and quality of life.
What is known already: Deficiency of pituitary gonadotropins (LH and FSH) due to hypogonadotropic hypogonadism (HH) can result in poor testicular development, low testicular volumes, micropenis and cryptorchidism. Inadequate hormonal replacement can lead to long-term issues, including subfertility or infertility, and reduced quality of life. Exogenous testosterone for pubertal induction can elevate serum testosterone concentrations and induce virilization, but it does not promote testicular development nor induce spermatogenesis. Fertility and testes growth remain primary concerns for patients seeking treatment.
Study design size duration: We conducted a retrospective observational review of male adolescents and young adults with gonadotropin deficiency and seeking puberty replacement therapy at two large tertiary centre hospitals in London, UK, from 2010 to 2024.
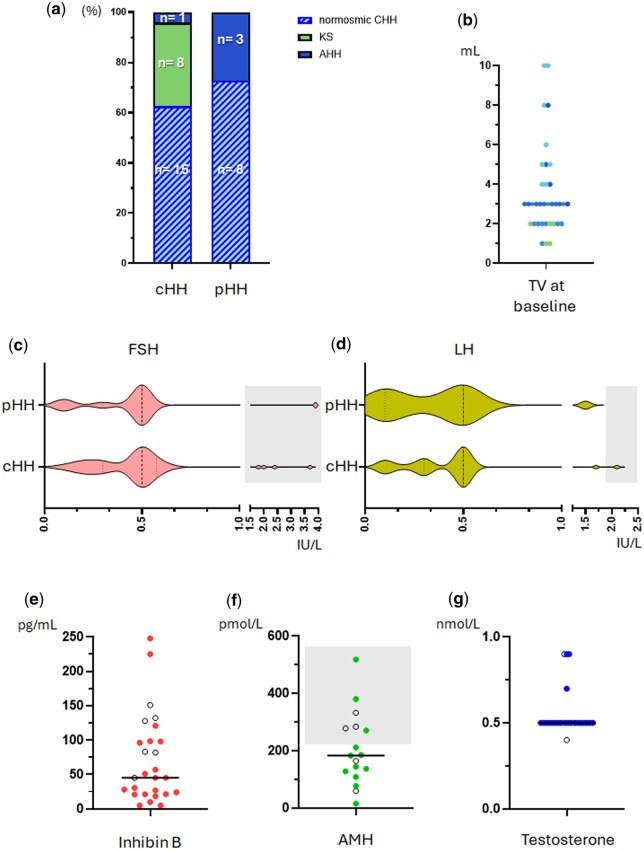
Participants/materials setting methods: A total of 35 males, with diagnosis of congenital hypogonadotropic hypogonadism (CHH: n = 23; further subdivided into those with partial [pHH: n = 8] and those with complete gonadotropin deficiency [cHH: n = 15]), acquired HH (AHH: n = 4) or Kallmann syndrome (KS: n = 8), received combined gonadotropin therapy. We assessed testicular growth and semen quality post-treatment.
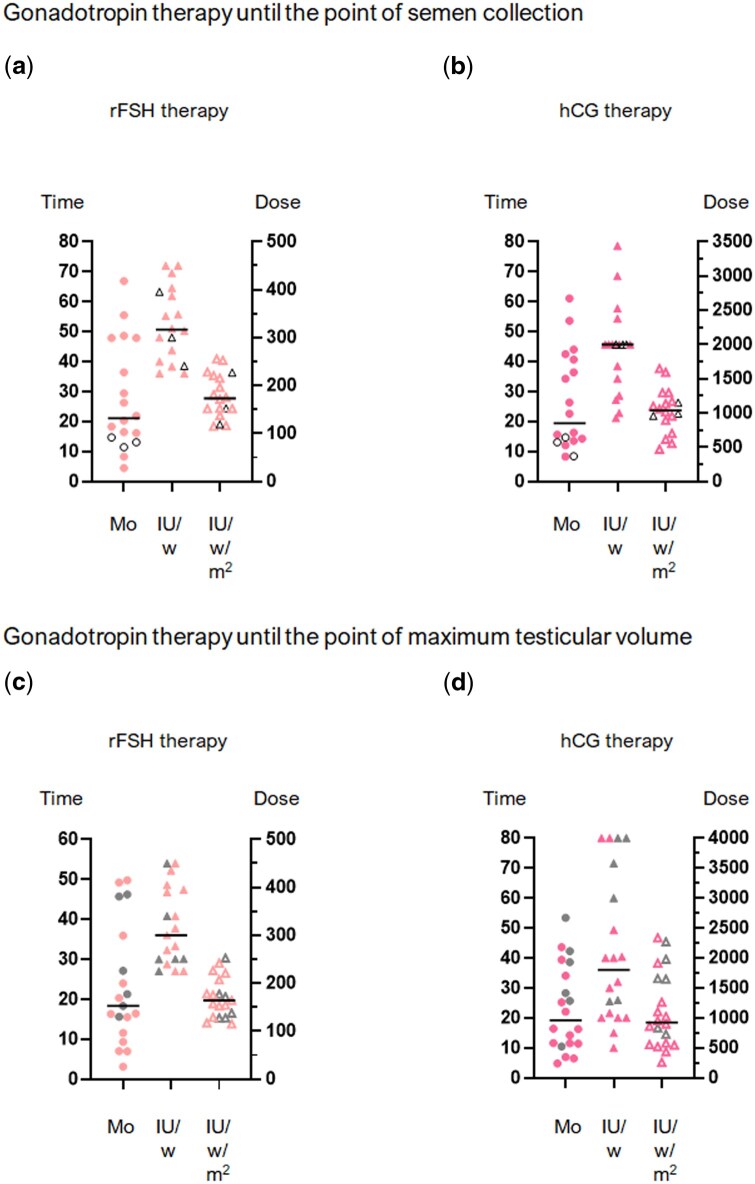
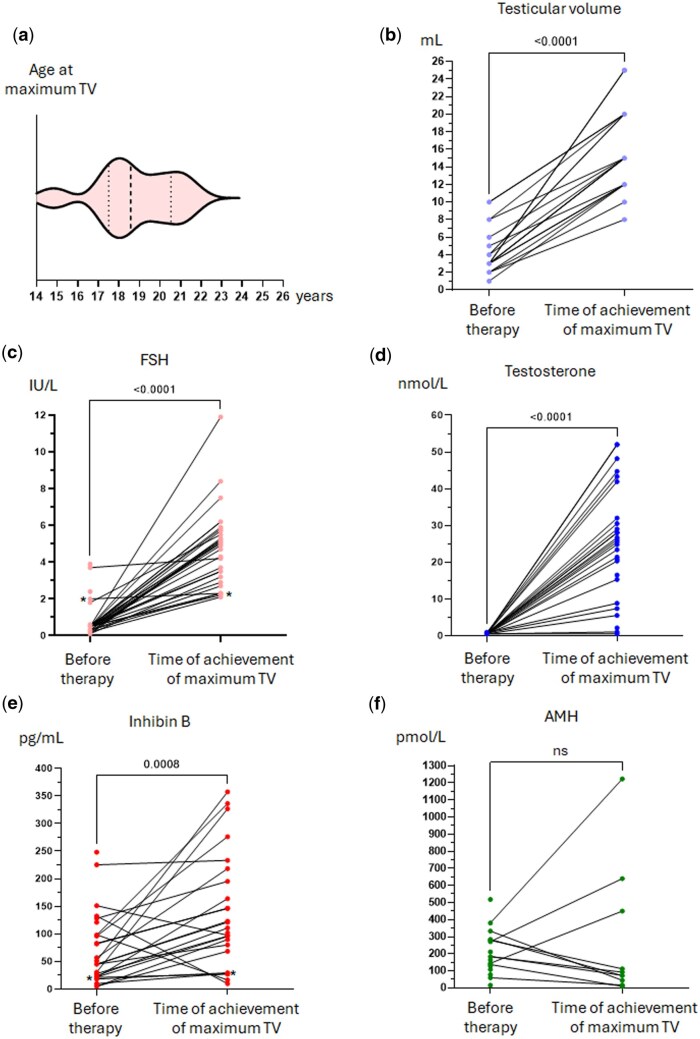
Main results and the role of chance: The majority of patients were referred for pubertal delay, alone or in combination with cryptorchidism, micropenis or microorchidism. Out of 35 patients, 22 (63%) had previously received testosterone, and the median age at gonadotropin treatment initiation was 15.8 years (range: 11.8-22.7). Semen analysis was obtained in 18 out of 19 patients who had received gonadotropin therapy for a median treatment duration of 21.1 months (range: 4.5-66.9) for rFSH and 19.5 months (range: 8.3-61.1) for hCG. The median sperm count on semen analysis was 8.9 × 106/ml (range: 0.0-54.9). Significant increases were noted in testicular volume (median change after therapy: 10.5 ml [95% CI 9.5-13.6], P < 0.0001), testosterone (median increase: 25.7 nmol/l [95% CI 19.8-31.5], P < 0.0001) and inhibin B levels (67.7 pg/ml [95% CI 18.4-86.7], P = 0.0008).
Limitations reasons for caution: The relatively low representation of patients with acquired HH in our study emphasizes the need to extrapolate the findings with caution in this specific subgroup of adolescent males with HH. The study is also an observational one, therefore meaning that some outcomes (such as change in inhibin B concentration) were not collected routinely and not reported for all patients. The observational nature of the study design also accounts for the differences in doses and duration observed in gonadotropin therapy.
Wider implications of the findings: The treatment of adult male infertility is particularly difficult in severe forms of gonadotropin deficiency, where there has been no testicular stimulation during mini-puberty or puberty. Appropriate hormonal replacement in puberty with combined gonadotropins can induce testicular maturation and spermatogenesis, but data are limited and at present, there is no international consensus on best practice regimens in adolescent and young adult males. Our treatment protocol induced testicular growth and caused increases in serum testosterone and Sertoli cell biomarkers, and spermatogenesis in 15/18 of patients who had completed semen analysis. This indicates the potential to substantially improve the reproductive, physical, and psychological health of patients who have a significant and unmet need for adequate hormonal replacement during puberty. The study described here included patients with diverse forms of HH (congenital, acquired, complete, and partial HH), thereby providing encouraging results across a variety of subjects with impaired puberty facing increased odds of fertility problems in adulthood. Additionally, we observed similar sperm counts between those who received exogenous testosterone treatment prior to gonadotropin therapy and those who began directly on gonadotropins for pubertal induction. This last finding is aligned with previous data and may help to reassure paediatric endocrinologists with limited access to rFSH or hCG that the use of exogenous testosterone to induce androgen-dependent changes in patients seeking treatment for pubertal delay is unlikely to compromise spermatogenic potential, should gonadotropins become available at a later stage.
Study funding/competing interests: S.C. was funded by an ESPE Early Career Scientific Development Grant. S.R.H. was funded by the Wellcome Trust (222049/Z/20/Z) and Barts Charity [MGU0552]. K.N.Y. was employed under the NIHR Specialist Foundation Programme. F.d.A. was funded by the student traineeship, University of Rome 'Tor Vergata', an Erasmus Grant and an ESPE Early Career Scientific Development Grant. E.C.A. was funded by an NIHR Academic Clinical Fellowship (ACF-2021-19-002). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care. G.B. received an ESPE Mid-Career Research Fellowship to enable the development of the clinical treatment schedule. The authors have no conflicting interests.
研究问题:重组FSH (rFSH)和hCG对促性腺激素缺乏症男性青少年和年轻人促进睾丸生长和精子发生有效吗?总结性回答:综合促性腺激素治疗在促性腺激素缺乏的男性青少年和年轻成人中诱导青春期和促进精子发生是有效的,并且有可能改善与生育和生活质量相关的成人结局。已知情况:由促性腺功能减退症(HH)引起的垂体促性腺激素(LH和FSH)缺乏可导致睾丸发育不良、睾丸体积小、小阴茎和隐睾。激素替代不足会导致长期问题,包括生育能力低下或不孕症,以及生活质量下降。外源性睾酮诱导青春期可提高血清睾酮浓度,诱导男性化,但不能促进睾丸发育,也不能诱导精子发生。对于寻求治疗的患者来说,生育能力和睾丸生长仍然是首要问题。研究设计规模持续时间:我们对2010年至2024年在英国伦敦两家大型三级中心医院接受促性腺激素缺乏症并寻求青春期替代疗法的男性青少年和年轻人进行了回顾性观察性回顾。参与者/材料设置方法:男性35例,诊断为先天性促性腺功能减退症(CHH: n = 23;进一步细分为部分[pHH: n = 8]和完全促性腺激素缺乏症[cHH: n = 15])、获得性HH (AHH: n = 4)或Kallmann综合征(KS: n = 8),接受促性腺激素联合治疗。我们评估了治疗后的睾丸生长和精液质量。主要结果及偶然性的作用:以青春期发育迟缓、单独或合并隐睾、小阴茎或小睾丸症患者居多。在35例患者中,22例(63%)先前接受过睾酮治疗,促性腺激素治疗开始时的中位年龄为15.8岁(范围:11.8-22.7)。在接受促性腺激素治疗的19例患者中,有18例进行了精液分析,其中rFSH的中位治疗持续时间为21.1个月(范围:4.5-66.9),hCG的中位治疗持续时间为19.5个月(范围:8.3-61.1)。精液分析中位精子数为8.9 × 106/ml(范围:0.0-54.9)。睾丸体积显著增加(治疗后中位变化:10.5 ml [95% CI 9.5-13.6], P P P = 0.0008)。谨慎的局限性原因:在我们的研究中,获得性HH患者的代表性相对较低,这强调了在青少年男性HH这一特定亚组中谨慎推断研究结果的必要性。该研究也是一项观察性研究,因此意味着一些结果(如抑制素B浓度的变化)没有常规收集,也没有报告所有患者。研究设计的观察性质也解释了促性腺激素治疗中剂量和持续时间的差异。研究结果的更广泛意义:治疗严重促性腺激素缺乏症的成年男性不育症尤其困难,在青春期或青春期没有睾丸刺激。在青春期适当的激素替代联合促性腺激素可以诱导睾丸成熟和精子发生,但数据有限,目前,对于青少年和年轻成年男性的最佳实践方案尚无国际共识。在完成精液分析的15/18的患者中,我们的治疗方案诱导了睾丸生长,并导致血清睾酮和支持细胞生物标志物的增加,以及精子发生。这表明,对于那些在青春期有显著且未满足足够激素替代需求的患者,有可能大幅改善生殖、身体和心理健康。本文描述的研究包括不同形式的HH患者(先天性,获得性,完全性和部分性HH),因此在青春期受损的各种受试者中提供了令人鼓舞的结果,这些受试者在成年后面临生育问题的几率增加。此外,我们观察到在促性腺激素治疗之前接受外源性睾酮治疗的患者和直接开始使用促性腺激素诱导青春期的患者精子数量相似。最后一项发现与先前的数据一致,并可能有助于使获得rFSH或hCG有限的儿科内分泌学家放心,使用外源性睾酮诱导寻求青春期延迟治疗的患者的雄激素依赖性变化不太可能损害生精潜力,如果在后期获得促性腺激素。研究经费/竞争利益:S.C.由ESPE早期职业科学发展基金资助。S.R.H.由惠康信托基金(222049/Z/20/Z)和巴茨慈善机构[MGU0552]资助。K.N.Y. 在国家卫生研究院专家基金计划下受聘。F.d.A.由学生实习、罗马大学“Tor Vergata”、伊拉斯谟基金和ESPE早期职业科学发展基金资助。e.c.a由NIHR学术临床奖学金(ACF-2021-19-002)资助。本出版物中表达的观点是作者的观点,不一定代表NIHR, NHS或英国卫生和社会保障部的观点。G.B.获得了ESPE中期职业研究奖学金,以促进临床治疗计划的发展。作者没有利益冲突。试验注册号:无。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


