Samaneh Salimian, Nathaniel Mark Hawkins, Nandini Dendukuri, Negareh Mousavi, James Brophy
{"title":"Predicting death or readmission following heart failure hospitalisation: the VancOuver CoastAL Acute Heart Failure (VOCAL-AHF) registry.","authors":"Samaneh Salimian, Nathaniel Mark Hawkins, Nandini Dendukuri, Negareh Mousavi, James Brophy","doi":"10.1136/openhrt-2025-003210","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart failure (HF) readmission and mortality rates remain high among HF patients. Improved and robust risk prediction models for better monitoring, informed decision-making, targeted interventions and improved patient outcomes are required. We developed and validated a patient-centric model to predict long-term outcomes of death or a repeat HF-hospitalisation using a modern model selection approach.</p><p><strong>Methods: </strong>We used data from a contemporary registry of patients discharged alive from an HF-hospitalisation between 1 April 2015 and 31 March 2019. An integrated and multifaceted selection approach (combining backward selection, least absolute shrinkage and selection operator and expert opinion) to Cox-proportional hazard models was used for model development. To account for model uncertainty and improve generalisability, bootstrap-Bayesian Model Averaging was used to derive the final risk model.</p><p><strong>Results: </strong>The cohort included 1842 patients with a median follow-up time of 529 days (range 2-1459 days). 790 (43%) patients experienced the outcome, with 68 (8.6%) having the outcome within 30 days. The final risk model included 12 variables, of which 8 were identified as being dominant. The top predictors with >99% probability for model inclusion were increasing age (HR 1.07, 95% CI 1.00 to 1.11/5 years), prior HF-diagnoses (1.47, 95% CI 1.13 to 1.71) and lower discharge haemoglobin (1.10, 95% CI 1.05 to 1.15/10 g/L). Other predictors (~>60% model-selection probability) included lower admitting systolic blood pressure, higher loop-diuretic discharge requirements, persistent smoking, an admitting non-sinus rhythm and absence of discharge angiotensin-converting enzyme inhibitor, angiotensin receptor blocker or angiotensin receptor-neprilysin inhibitor prescription. The 3-year cross-validated c-statistic was 0.63 (95% CI 0.61 to 0.65).</p><p><strong>Conclusions: </strong>A clinically oriented prognostic model with moderate discrimination, to predict adverse events postdischarge for HF, has been developed and internally validated. This model, leveraging an integrated approach to selection, shows promise in personalising discharge planning. Future external validation is necessary to confirm its applicability and potential impact on clinical practice.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142106/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Heart failure (HF) readmission and mortality rates remain high among HF patients. Improved and robust risk prediction models for better monitoring, informed decision-making, targeted interventions and improved patient outcomes are required. We developed and validated a patient-centric model to predict long-term outcomes of death or a repeat HF-hospitalisation using a modern model selection approach.
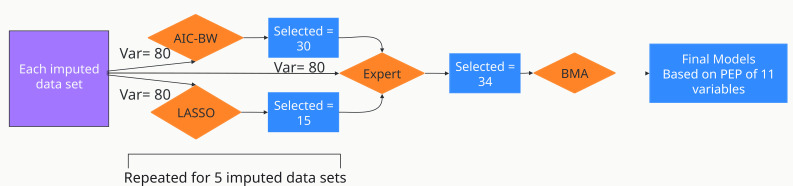
Methods: We used data from a contemporary registry of patients discharged alive from an HF-hospitalisation between 1 April 2015 and 31 March 2019. An integrated and multifaceted selection approach (combining backward selection, least absolute shrinkage and selection operator and expert opinion) to Cox-proportional hazard models was used for model development. To account for model uncertainty and improve generalisability, bootstrap-Bayesian Model Averaging was used to derive the final risk model.
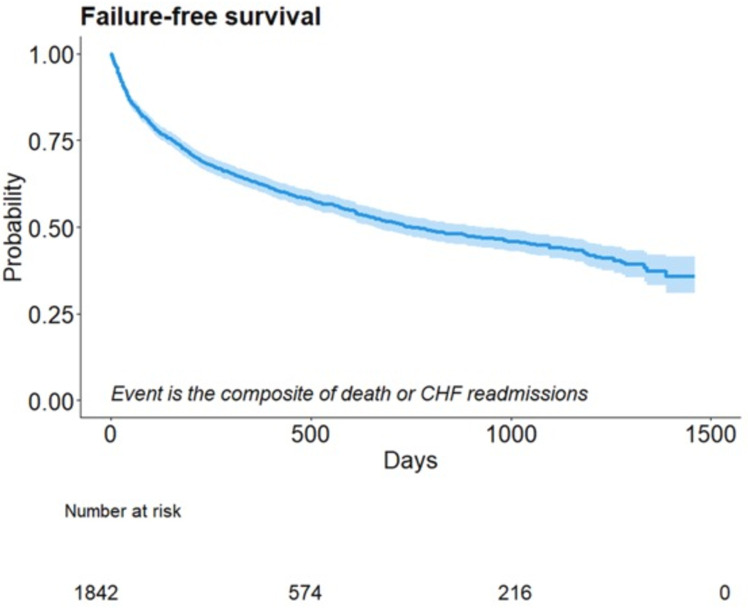
Results: The cohort included 1842 patients with a median follow-up time of 529 days (range 2-1459 days). 790 (43%) patients experienced the outcome, with 68 (8.6%) having the outcome within 30 days. The final risk model included 12 variables, of which 8 were identified as being dominant. The top predictors with >99% probability for model inclusion were increasing age (HR 1.07, 95% CI 1.00 to 1.11/5 years), prior HF-diagnoses (1.47, 95% CI 1.13 to 1.71) and lower discharge haemoglobin (1.10, 95% CI 1.05 to 1.15/10 g/L). Other predictors (~>60% model-selection probability) included lower admitting systolic blood pressure, higher loop-diuretic discharge requirements, persistent smoking, an admitting non-sinus rhythm and absence of discharge angiotensin-converting enzyme inhibitor, angiotensin receptor blocker or angiotensin receptor-neprilysin inhibitor prescription. The 3-year cross-validated c-statistic was 0.63 (95% CI 0.61 to 0.65).
Conclusions: A clinically oriented prognostic model with moderate discrimination, to predict adverse events postdischarge for HF, has been developed and internally validated. This model, leveraging an integrated approach to selection, shows promise in personalising discharge planning. Future external validation is necessary to confirm its applicability and potential impact on clinical practice.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


