Merve Süleyman, Deniz Cagdas, Pelin Özlem Şimşek Kiper, Gülen Eda Ütine, Merve Kaşıkcı Çavdar, Feyzi İlhan Tezcan
{"title":"Clinical and Immunological Features of a Large DiGeorge Syndrome Cohort.","authors":"Merve Süleyman, Deniz Cagdas, Pelin Özlem Şimşek Kiper, Gülen Eda Ütine, Merve Kaşıkcı Çavdar, Feyzi İlhan Tezcan","doi":"10.1007/s10875-025-01884-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>DiGeorge Syndrome (DGS), a microdeletion syndrome, shows a broad spectrum from mild T-cell lymphopenia to severe combined immunodeficiency.</p><p><strong>Aim: </strong>To define the clinical/immunophenotypical biomarkers for DGS.</p><p><strong>Patients and methods: </strong>A total of 72 patients with 22q11.2 deletion(n = 66) and those fulfilling the DGS criteria without deletion (n = 6) were enrolled.</p><p><strong>Results: </strong>The male/female ratio was 41/31. Median age at clinical diagnosis was 1.7 years (0 days-22 years) with follow-up for 21.7 months (0 days-17.3 years). Common evaluation reasons were cardiac features (30.6%), failure to thrive (15.3%), and neurological features (15.3%). Craniofacial dysmorphism (64/66, 97%), central nervous system findings (62/72, 86.1%), and congenital cardiovascular defect (43/70, 61.4%) were common. We noted lymphopenia (30/72, 41.7%) and low IgM (25/69, 36.2%). T helper cell counts were low in 49.3% (33/67). T cytotoxic and NK cell counts were normal/high in 80.6% (54/67) and 97% (65/67) of patients, respectively. 42.3% (11/26) had low CD4 + TEMRA, and 34.6% (9/26) had low CD8 + TEM percentages. None had low CD8 + TEMRA. B cells were normal/high (52/67, 77.6%). 30.8%(8/26) had low switched-memory and 38.5% (10/26) had low active B cell percentages. Low IgA levels were associated with decreased lymphocyte activation and recent thymic emigrant (RTE) cell percentages. Six(8.3%) patients with lymphopenia, three of whom had congenital athymia, died.</p><p><strong>Conclusion: </strong>CD4 lymphopenia was more common than CD8 lymphopenia. Normal/high CD8 + and NK cell counts were remarkable. Increased CD8+ TEMRA cells seem to indicate peripheral homeostatic proliferation following viral infections. Low serum IgA correlated with low RTE% and impaired T-cell function. DGS severity markers include hypocalcemia, congenital cardiac anomaly, and T-cell lymphopenia.</p>","PeriodicalId":15531,"journal":{"name":"Journal of Clinical Immunology","volume":"45 1","pages":"103"},"PeriodicalIF":5.7000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12133924/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10875-025-01884-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: DiGeorge Syndrome (DGS), a microdeletion syndrome, shows a broad spectrum from mild T-cell lymphopenia to severe combined immunodeficiency.
Aim: To define the clinical/immunophenotypical biomarkers for DGS.
Patients and methods: A total of 72 patients with 22q11.2 deletion(n = 66) and those fulfilling the DGS criteria without deletion (n = 6) were enrolled.
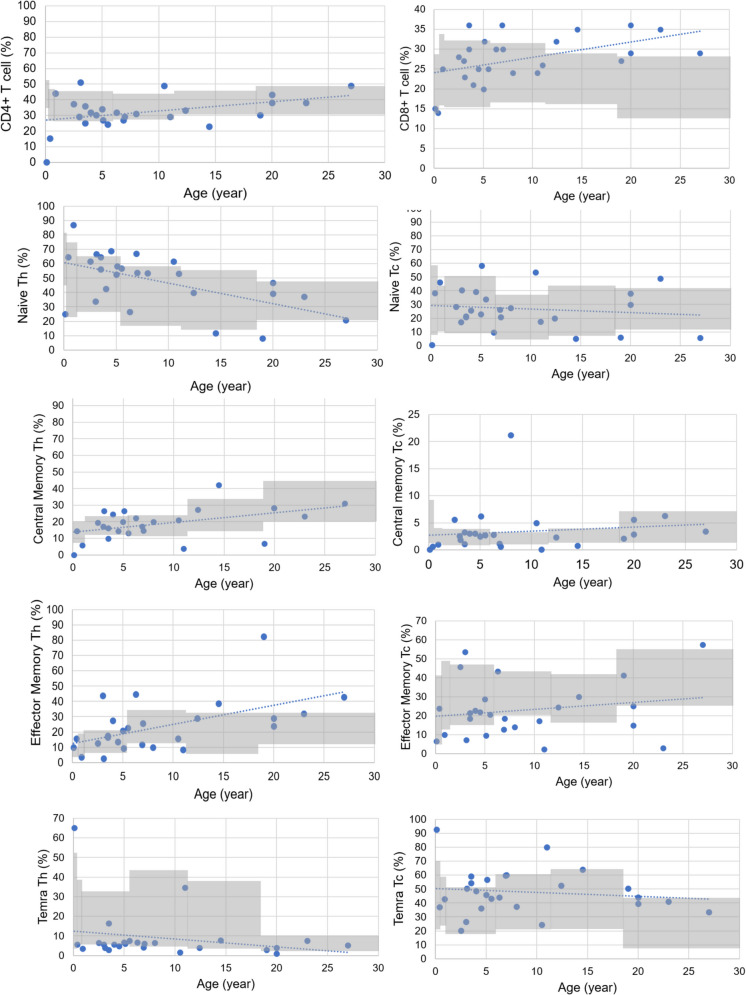
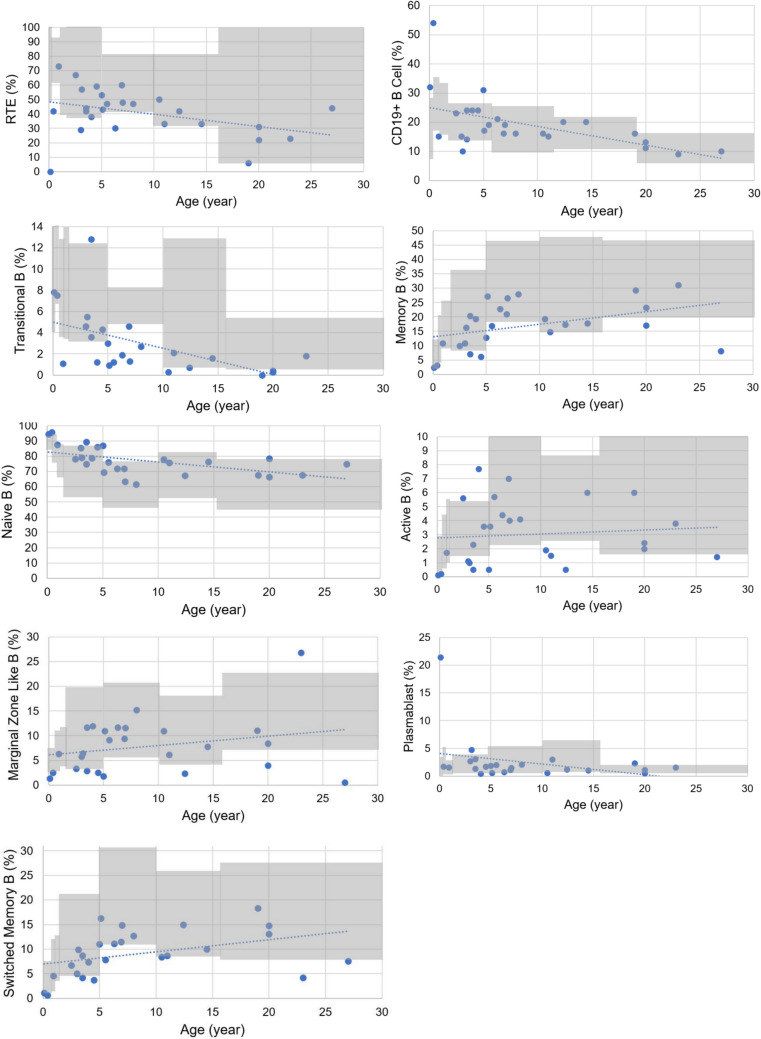
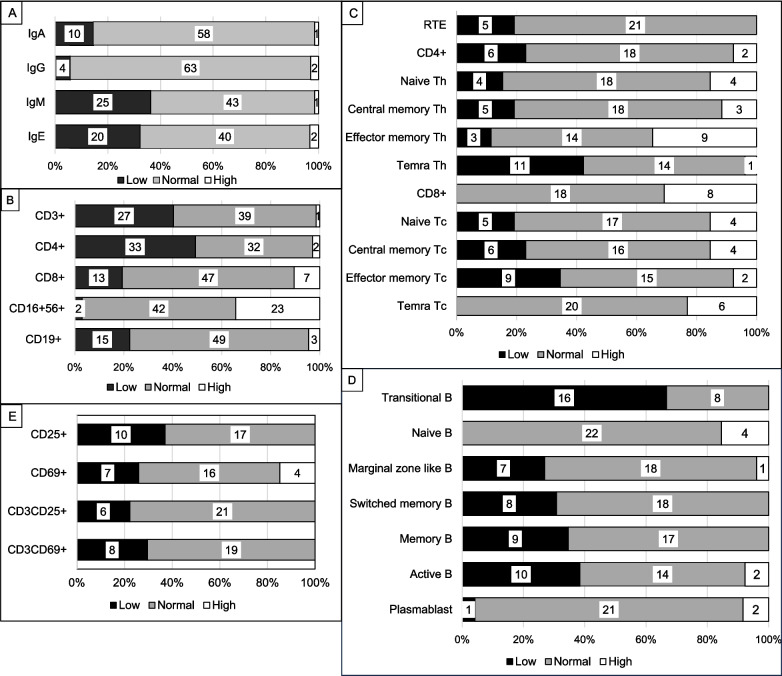
Results: The male/female ratio was 41/31. Median age at clinical diagnosis was 1.7 years (0 days-22 years) with follow-up for 21.7 months (0 days-17.3 years). Common evaluation reasons were cardiac features (30.6%), failure to thrive (15.3%), and neurological features (15.3%). Craniofacial dysmorphism (64/66, 97%), central nervous system findings (62/72, 86.1%), and congenital cardiovascular defect (43/70, 61.4%) were common. We noted lymphopenia (30/72, 41.7%) and low IgM (25/69, 36.2%). T helper cell counts were low in 49.3% (33/67). T cytotoxic and NK cell counts were normal/high in 80.6% (54/67) and 97% (65/67) of patients, respectively. 42.3% (11/26) had low CD4 + TEMRA, and 34.6% (9/26) had low CD8 + TEM percentages. None had low CD8 + TEMRA. B cells were normal/high (52/67, 77.6%). 30.8%(8/26) had low switched-memory and 38.5% (10/26) had low active B cell percentages. Low IgA levels were associated with decreased lymphocyte activation and recent thymic emigrant (RTE) cell percentages. Six(8.3%) patients with lymphopenia, three of whom had congenital athymia, died.
Conclusion: CD4 lymphopenia was more common than CD8 lymphopenia. Normal/high CD8 + and NK cell counts were remarkable. Increased CD8+ TEMRA cells seem to indicate peripheral homeostatic proliferation following viral infections. Low serum IgA correlated with low RTE% and impaired T-cell function. DGS severity markers include hypocalcemia, congenital cardiac anomaly, and T-cell lymphopenia.
期刊介绍:
The Journal of Clinical Immunology publishes impactful papers in the realm of human immunology, delving into the diagnosis, pathogenesis, prognosis, or treatment of human diseases. The journal places particular emphasis on primary immunodeficiencies and related diseases, encompassing inborn errors of immunity in a broad sense, their underlying genotypes, and diverse phenotypes. These phenotypes include infection, malignancy, allergy, auto-inflammation, and autoimmunity. We welcome a broad spectrum of studies in this domain, spanning genetic discovery, clinical description, immunologic assessment, diagnostic approaches, prognosis evaluation, and treatment interventions. Case reports are considered if they are genuinely original and accompanied by a concise review of the relevant medical literature, illustrating how the novel case study advances the field. The instructions to authors provide detailed guidance on the four categories of papers accepted by the journal.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


