Factors associated with symptom-to-surgery time in patients undergoing surgical repair for acute type A aortic dissection: an exploratory analysis from a prospective cohort study.
Wilson Fandino, Tom Gilbey, Benjamin Milne, Joe Arrowsmith, Seema Agarwal, Matthew Dodd, Tim C Clayton, Gudrun Kunst
{"title":"Factors associated with symptom-to-surgery time in patients undergoing surgical repair for acute type A aortic dissection: an exploratory analysis from a prospective cohort study.","authors":"Wilson Fandino, Tom Gilbey, Benjamin Milne, Joe Arrowsmith, Seema Agarwal, Matthew Dodd, Tim C Clayton, Gudrun Kunst","doi":"10.1136/bmjsit-2024-000304","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong></p><p><strong>Objectives: </strong>The primary objective of this study was to investigate perioperative factors associated with symptom-to-surgery (STS) time in patients diagnosed with hyper-acute aortic dissection (AAD). The secondary objective was to develop a causal model to understand the relationship between STS times and hospital mortality in this population.</p><p><strong>Design: </strong>Prospective cohort study.</p><p><strong>Setting: </strong>Exploratory analysis of a national audit conducted by the Association of Cardiothoracic Anaesthesia and Critical Care.</p><p><strong>Participants: </strong>From a total of 270 participants diagnosed with AAD with an STS time <72 hours, 218 were included in the multivariate analysis, after excluding 52 participants with missing covariates.</p><p><strong>Main outcome measures: </strong>STS time, measured in hours. Hospital mortality at 30 days.</p><p><strong>Results: </strong>In the multivariate analysis, mean STS time for misdiagnosed patients was nearly twice as high when compared with patients who initially had the correct diagnosis (estimated proportion of change=1.9, 95% CI 1.5 to 2.3, p<0.001). STS time decreased when patients were accompanied by a medical doctor in the ambulance transfer, had mean arterial blood pressure below 70 mm Hg or presented to the emergency department (ED) with a Glasgow Coma Scale (GCS) <15. Estimated ED-to-surgery (ETS) times were 1.8 hours longer for women than for men (10.5 hours, 95% CI 9.0 to 12.0 hours vs 8.7 hours, 95% CI 7.8 to 9.6 hours). From a total of 334 patients, 64 (19.2%) died. Mortality was higher in older patients and when STS time was ≥6 and <24 hours, compared with STS time <6 hours.</p><p><strong>Conclusions: </strong>Potentially modifiable factors that may reduce STS times include avoidance of misdiagnosis and provision of a medical doctor for the ambulance transfer. Younger women had longer STS and ETS times, but further research is warranted to investigate the impact of age and sex on these times. The relationship between STS time and hospital mortality among these patients remains unclear.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"7 1","pages":"e000304"},"PeriodicalIF":1.6000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121560/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2024-000304","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Abstract:
Objectives: The primary objective of this study was to investigate perioperative factors associated with symptom-to-surgery (STS) time in patients diagnosed with hyper-acute aortic dissection (AAD). The secondary objective was to develop a causal model to understand the relationship between STS times and hospital mortality in this population.
Design: Prospective cohort study.
Setting: Exploratory analysis of a national audit conducted by the Association of Cardiothoracic Anaesthesia and Critical Care.
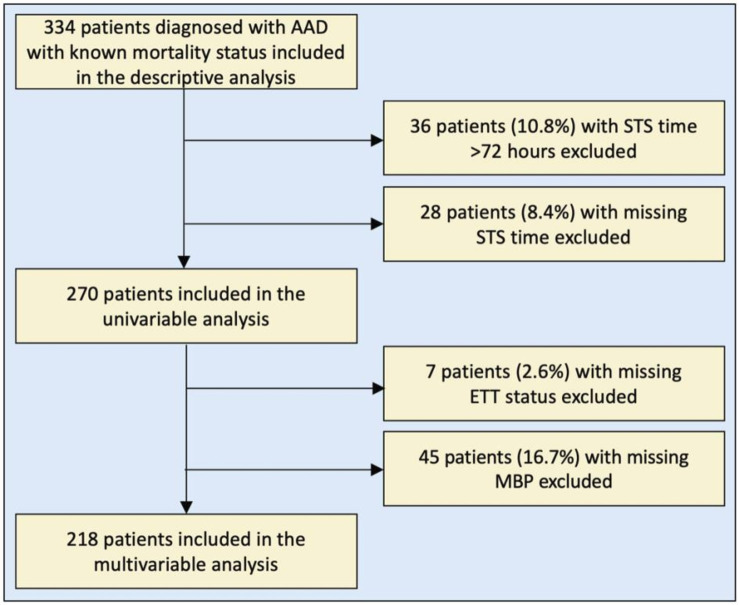
Participants: From a total of 270 participants diagnosed with AAD with an STS time <72 hours, 218 were included in the multivariate analysis, after excluding 52 participants with missing covariates.
Main outcome measures: STS time, measured in hours. Hospital mortality at 30 days.
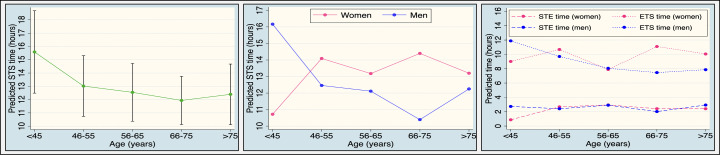
Results: In the multivariate analysis, mean STS time for misdiagnosed patients was nearly twice as high when compared with patients who initially had the correct diagnosis (estimated proportion of change=1.9, 95% CI 1.5 to 2.3, p<0.001). STS time decreased when patients were accompanied by a medical doctor in the ambulance transfer, had mean arterial blood pressure below 70 mm Hg or presented to the emergency department (ED) with a Glasgow Coma Scale (GCS) <15. Estimated ED-to-surgery (ETS) times were 1.8 hours longer for women than for men (10.5 hours, 95% CI 9.0 to 12.0 hours vs 8.7 hours, 95% CI 7.8 to 9.6 hours). From a total of 334 patients, 64 (19.2%) died. Mortality was higher in older patients and when STS time was ≥6 and <24 hours, compared with STS time <6 hours.
Conclusions: Potentially modifiable factors that may reduce STS times include avoidance of misdiagnosis and provision of a medical doctor for the ambulance transfer. Younger women had longer STS and ETS times, but further research is warranted to investigate the impact of age and sex on these times. The relationship between STS time and hospital mortality among these patients remains unclear.
摘要:目的:本研究的主要目的是探讨超急性主动脉夹层(AAD)患者围手术期与症状到手术(STS)时间相关的因素。次要目的是建立一个因果模型,以了解STS时间与该人群住院死亡率之间的关系。设计:前瞻性队列研究。背景:由心胸麻醉和危重症护理协会进行的国家审计的探索性分析。参与者:共270名诊断为AAD且STS时间的参与者。主要结果测量:STS时间,以小时计。30天住院死亡率结果:在多变量分析中,与最初诊断正确的患者相比,误诊患者的平均STS时间几乎是其两倍(估计变化比例=1.9,95% CI 1.5至2.3)。结论:可能减少STS时间的潜在可修改因素包括避免误诊和为救护车转移提供医生。年轻女性的STS和ETS时间较长,但需要进一步研究年龄和性别对这些时间的影响。这些患者的STS时间与住院死亡率之间的关系尚不清楚。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


