Primary Prophylaxis for High-Risk Varices in Patients with Hepatocellular Carcinoma and Portal Vein Tumor Thrombus Delayed Hepatic Decompensation: A Retrospective, Propensity Score Matching Study.
{"title":"Primary Prophylaxis for High-Risk Varices in Patients with Hepatocellular Carcinoma and Portal Vein Tumor Thrombus Delayed Hepatic Decompensation: A Retrospective, Propensity Score Matching Study.","authors":"Yu-Jen Chen, Ming-Chih Hou, Tsung-Chieh Yang, Pei-Chang Lee, Hsiao-Sheng Lu, Hui-Chun Huang, Yi-Hsiang Huang, Jiing-Chyuan Luo","doi":"10.2147/JHC.S520318","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>The prevalence of clinically significant portal hypertension (CSPH) is high in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT). There was no evidence of whether primary prophylaxis is beneficial in reducing hepatic decompensation in these patients.</p><p><strong>Methods: </strong>Clinical records of 445 patients with pathology or radiology-confirmed HCC and PVTT from January 2013 to December 2022 were reviewed, 142 patients having concurrent high-risk varices (HRV) without hepatic decompensation were enrolled. Patients were divided into the prophylaxis group and non-prophylaxis group. Propensity score matching was used for group comparison. The primary endpoint was decompensation-free survival (DFS), and the secondary endpoints were the incidence of esophageal variceal bleeding (EVB) and overall survival (OS).</p><p><strong>Results: </strong>The incidence of EVB was higher in the non-prophylaxis group than in the prophylaxis group (46.8% VS 21%, p = 0.001). DFS was longer in the prophylaxis group than in the non-prophylaxis group (84 days vs 66 days, p = 0.009). There was no difference in OS between two groups. In multivariate analysis, primary prophylaxis was associated with longer DFS (HR 0.806, p = 0.017); Immunotherapy (IO) was associated with longer DFS and OS; Barcelona Clinic Liver Cancer (BCLC) stage D was associated with shorter DFS and OS.</p><p><strong>Conclusion: </strong>Primary prophylaxis delays hepatic decompensation in HCC patients with PVTT. The incidence of EVB was also lower in the prophylaxis group, particularly in those treated with NSBB. First-line IO treatment is independently associated with better DFS and OS.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1057-1067"},"PeriodicalIF":3.4000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12127523/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S520318","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: The prevalence of clinically significant portal hypertension (CSPH) is high in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT). There was no evidence of whether primary prophylaxis is beneficial in reducing hepatic decompensation in these patients.
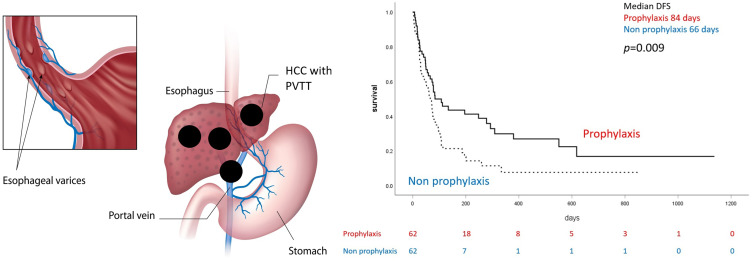
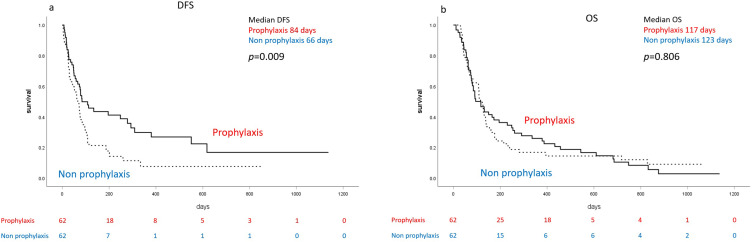
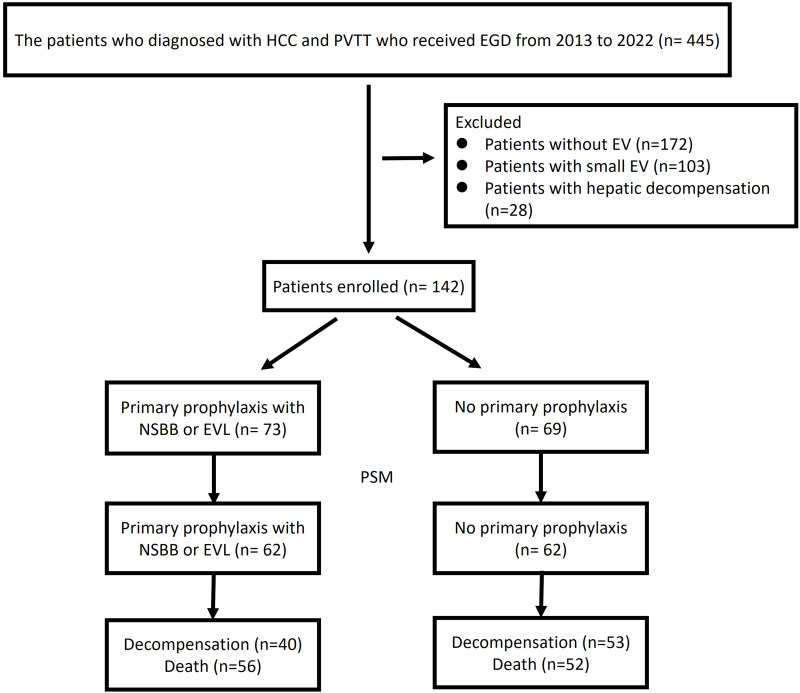
Methods: Clinical records of 445 patients with pathology or radiology-confirmed HCC and PVTT from January 2013 to December 2022 were reviewed, 142 patients having concurrent high-risk varices (HRV) without hepatic decompensation were enrolled. Patients were divided into the prophylaxis group and non-prophylaxis group. Propensity score matching was used for group comparison. The primary endpoint was decompensation-free survival (DFS), and the secondary endpoints were the incidence of esophageal variceal bleeding (EVB) and overall survival (OS).
Results: The incidence of EVB was higher in the non-prophylaxis group than in the prophylaxis group (46.8% VS 21%, p = 0.001). DFS was longer in the prophylaxis group than in the non-prophylaxis group (84 days vs 66 days, p = 0.009). There was no difference in OS between two groups. In multivariate analysis, primary prophylaxis was associated with longer DFS (HR 0.806, p = 0.017); Immunotherapy (IO) was associated with longer DFS and OS; Barcelona Clinic Liver Cancer (BCLC) stage D was associated with shorter DFS and OS.
Conclusion: Primary prophylaxis delays hepatic decompensation in HCC patients with PVTT. The incidence of EVB was also lower in the prophylaxis group, particularly in those treated with NSBB. First-line IO treatment is independently associated with better DFS and OS.
背景与目的:肝细胞癌(HCC)和门静脉肿瘤血栓(PVTT)患者临床显著性门静脉高压症(CSPH)患病率高。没有证据表明初级预防是否有利于减少这些患者的肝功能失代偿。方法:回顾2013年1月至2022年12月445例病理或影像学证实的HCC和PVTT患者的临床资料,其中142例合并高危静脉曲张(HRV),无肝代偿。患者分为预防组和非预防组。采用倾向评分匹配进行组间比较。主要终点为无失代偿生存期(DFS),次要终点为食管静脉曲张出血(EVB)发生率和总生存期(OS)。结果:非预防组EVB发病率高于预防组(46.8% VS 21%, p = 0.001)。预防组的DFS比非预防组长(84天vs 66天,p = 0.009)。两组间OS无差异。在多变量分析中,初级预防与较长的DFS相关(HR 0.806, p = 0.017);免疫治疗(IO)与更长的DFS和OS相关;巴塞罗那临床肝癌(BCLC) D期与较短的DFS和OS相关。结论:初级预防可延缓肝细胞癌合并PVTT患者肝功能失代偿。预防组EVB的发病率也较低,特别是在接受NSBB治疗的组中。一线IO治疗与更好的DFS和OS独立相关。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


