Jirka Taylor, Sachini Bandara, Cindy Parks Thomas, Brendan Saloner, Peter James Fredericks, Karen Shen
{"title":"Predictors of non-transport by emergency medical services after a nonfatal opioid overdose: a national analysis.","authors":"Jirka Taylor, Sachini Bandara, Cindy Parks Thomas, Brendan Saloner, Peter James Fredericks, Karen Shen","doi":"10.1093/haschl/qxaf101","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Emergency medical services (EMS) response to nonfatal overdoses represents an opportunity to provide linkage to services. However, patients may decline follow-on transportation. This paper examined predictors associated with non-transport after nonfatal opioid overdoses.</p><p><strong>Methods: </strong>We undertook a cross-sectional analysis of 2021-2022 data from the National EMS Information System. The outcome was a binary measure of declined transport. Predictors included age, gender, race/ethnicity, response time, EMS level of care, naloxone does, setting, urbanicity, region, time, and day.</p><p><strong>Results: </strong>We identified 710 263 nonfatal opioid overdose events, of which 12.4% ended in non-transport. Men were more likely to decline transport (average marginal effect [AME] 0.020 [95% CI, 0.019-0.022]), and Black patients were less likely to decline (AME -0.022 [95% CI, -0.024 to -0.021]). Compared with events involving an EMS-administered limited first dose (<2 mg), non-transports were more likely in events without naloxone administration (AME 0.075 [95% CI, 0.073-0.078]), with administration only by laypersons (AME 0.101 [95% CI, 0.096-0.107]), and when EMS administered higher first doses (2-4 mg AME 0.039 [95% CI, 0.037-0.041]; 4 mg+ AME 0.053 [95% CI, 0.049-0.056]).</p><p><strong>Conclusion: </strong>Efforts to improve post-overdose care should focus on groups who are more likely to decline transport and on appropriate naloxone dosing.</p>","PeriodicalId":94025,"journal":{"name":"Health affairs scholar","volume":"3 5","pages":"qxaf101"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12123062/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health affairs scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/haschl/qxaf101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Emergency medical services (EMS) response to nonfatal overdoses represents an opportunity to provide linkage to services. However, patients may decline follow-on transportation. This paper examined predictors associated with non-transport after nonfatal opioid overdoses.
Methods: We undertook a cross-sectional analysis of 2021-2022 data from the National EMS Information System. The outcome was a binary measure of declined transport. Predictors included age, gender, race/ethnicity, response time, EMS level of care, naloxone does, setting, urbanicity, region, time, and day.
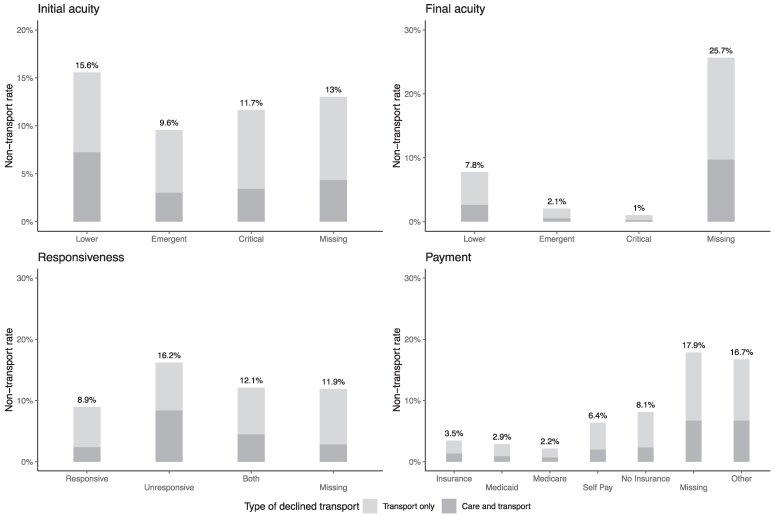
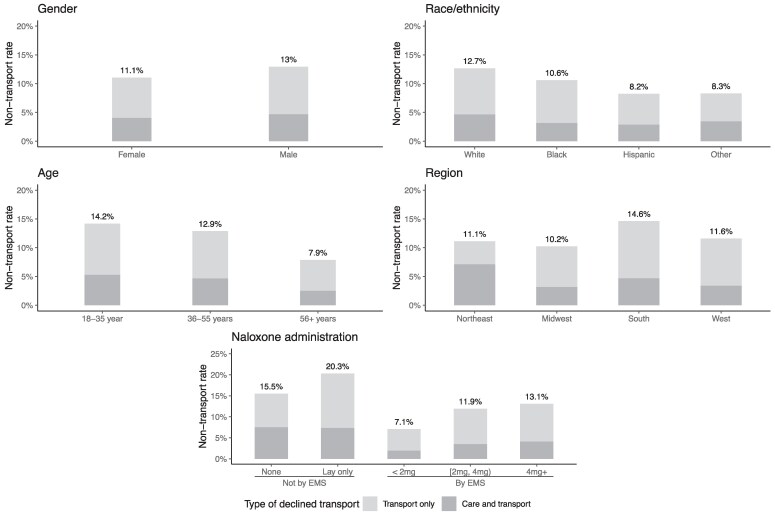
Results: We identified 710 263 nonfatal opioid overdose events, of which 12.4% ended in non-transport. Men were more likely to decline transport (average marginal effect [AME] 0.020 [95% CI, 0.019-0.022]), and Black patients were less likely to decline (AME -0.022 [95% CI, -0.024 to -0.021]). Compared with events involving an EMS-administered limited first dose (<2 mg), non-transports were more likely in events without naloxone administration (AME 0.075 [95% CI, 0.073-0.078]), with administration only by laypersons (AME 0.101 [95% CI, 0.096-0.107]), and when EMS administered higher first doses (2-4 mg AME 0.039 [95% CI, 0.037-0.041]; 4 mg+ AME 0.053 [95% CI, 0.049-0.056]).
Conclusion: Efforts to improve post-overdose care should focus on groups who are more likely to decline transport and on appropriate naloxone dosing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


