Stephanie K Y Choi, Wentao Li, Christos Venetis, William Ledger, Kei Lui, Katie Harris, Robert J Norman, Louisa R Jorm, Georgina M Chambers
{"title":"Perinatal risks associated with infertility and medically assisted reproduction: a population-based cohort study.","authors":"Stephanie K Y Choi, Wentao Li, Christos Venetis, William Ledger, Kei Lui, Katie Harris, Robert J Norman, Louisa R Jorm, Georgina M Chambers","doi":"10.1093/hropen/hoaf020","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Are the risks of adverse perinatal outcomes in singletons born from medically assisted reproduction (MAR) mainly associated with underlying parental infertility, or are they primarily linked to the MAR treatments?</p><p><strong>Summary answer: </strong>While MAR-conceived singletons have increased risks of preterm birth, admission to neonatal intensive care unit (NICU), and hospital admission in early life, these risks are mainly associated with the underlying parental infertility that led to the use of MAR technologies.</p><p><strong>What is known already: </strong>Children born from MAR are at increased risk for some adverse perinatal and infant outcomes. However, to what extent this risk is associated with infertility or MAR treatment remains unclear. This knowledge gap arises from the challenge in disentangling the effects of infertility and MAR treatment, given that parental infertility necessitates the use of MAR treatment.</p><p><strong>Study design size duration: </strong>This is a statewide longitudinally data-linked population-based cohort study conducted in New South Wales, Australia, involving all singleton infants born (liveborn or stillborn) between 2009 and 2017.</p><p><strong>Participants/materials setting methods: </strong>We applied two comparisons to isolate the associations of infertility from its treatment: (i) MAR infants versus naturally conceived infants from fertile parents (NC-fertile), and (ii) MAR infants versus naturally conceived infants from parents who had a history of infertility (NC-infertile). The study cohort consisted of 824 639 singleton infants, of whom 27 796 (3.4%) were conceived through ART and 13 574 (1.6%) through ovulation induction/intrauterine insemination (OI/IUI), while 783 269 (95.0%) of the infants were naturally conceived (747 018 NC-fertile controls and 36 251 NC-infertile controls). We used the inverse probability of treatment weighting method to make MAR infants comparable with each of the two NC control groups. We then calculated the adjusted risk differences (aRDs) in these propensity score-weighted cohorts. In the subgroup analyses of different forms of ART treatment (ICSI vs IVF and fresh vs frozen embryo transfer), we reweighted the study cohort and compared these subgroups with the two NC control groups separately.</p><p><strong>Main results and the role of chance: </strong>Singletons conceived through ART had a higher risk for preterm birth (aRD 25.7 per 1000 infants, 95% CI 21.3-30.0), admission to NICU (aRD 8.4 per 1000 infants, 95% CI 1.2-15.6), and hospital admission within 2 years of life (aRD 24.6 per 1000 infants, 95% CI 17.2-32.0) compared to NC-fertile controls. These risks were notably reduced when compared to NC-infertile controls (aRD 9.5 per 1000 infants, 95% CI 4.8-14.2 for preterm birth; -0.7 per 1000 infants, 95% CI -8.0 to 6.6 for NICU admission; and 10.6 per 1000 infants, 95% CI 2.5-18.7 for hospital admission within 2 years of life). ART-conceived singletons also had a higher risk of stillbirth compared to NC-fertile controls (aRD 1.5 per 1000 infants, 95% CI 0.4-2.7), which decreased when compared to NC-infertile controls (aRD 0.8 per 1000 infants, 95% CI -0.4 to 2.1). Similar patterns were observed for OI/IUI-conceived infants.Compared to NC-fertile controls, infants conceived by either ICSI (preterm birth: aRD 18.4 per 1000 infants, 95% CI 11.9-24.8; hospital admission: aRD 43.4 per 1000 infants, 95% CI 31.4-55.4) or IVF (preterm birth: aRD 26.4 per 1000 infants, 95% CI 18.7-34.1; hospital admission: aRD 30.2 per 1000 infants, 95% CI 17.0-43.4) had higher risks, but these risks decreased significantly when compared to NC-infertile controls (ICSI: preterm birth aRD 7.7 per 1000 infants, 95% CI 1.9-13.5; hospital admission aRD 17.0 per 1000 infants, 95% CI 6.9-27.2; IVF: preterm birth aRD 13.1 per 1000 infants, 95% CI 6.6-19.7; hospital admission aRD 0.9 per 1000 infants, 95% CI -10.3 to 12.0).Infants conceived by fresh ART transfers had higher risks of preterm birth (aRD 33.7 per 1000 infants, 95% CI 27.6-39.9) and hospital admission (aRD 33.7 per 1000 infants, 95% CI 23.5-43.9) compared to NC-fertile controls, with reduced risks when compared to NC-infertile controls (preterm birth: aRD 20.5 per 1000 infants, 95% CI 14.1-26.9; hospital admission: aRD 17.8 per 1000 infants, 95% CI 7.3-28.3). These risks were substantially lower for those conceived by frozen embryo transfers and came close to zero when compared to NC-infertile controls. However, frozen embryo transfer increased the risks of LGA (aRD 28.5 per 1000 infants, 95% CI 20.5-36.6) compared to NC-fertile controls, and this risk persisted when compared to NC-infertile controls.</p><p><strong>Limitations reasons for caution: </strong>The observational nature and use of administrative data may carry a risk of misclassification or unmeasured confounding. We only included singletons because the risk profile for multiple births differs significantly. Parents with a history of infertility who achieved natural pregnancy likely had less severe conditions, potentially underestimating the contribution of parental infertility to perinatal risks.</p><p><strong>Wider implications of the findings: </strong>The primary factor contributing to the increased risks of certain adverse perinatal outcomes is the underlying parental infertility that necessitates ART treatment. However, ART procedures also contribute to the risks to some extent; this study highlights the importance of careful monitoring and of reserving ART for where ART treatment is indicated.</p><p><strong>Study funding/competing interests: </strong>This study is funded by the Australian National Health and Medical Research Council (APP1127437). The sponsors had no role in: the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. S.K.Y.C. is an employee of Sanofi, but this study was conducted before this role. W.L. declared research grant support from the Australian National Health and Medical Research Council for other projects. C.V. declared having received honoraria for invited lectures in scientific meetings/conferences, and/or having travel support, and/or being a member of advisory boards for Merck Ltd, Merck Sharpe & Dohme, Ferring, Organon, Vianex, Gedeon-Richter, and IBSA. C.V. was a minority shareholder of Virtus Health Ltd until June 2022 and a member of the Board of Directors of the Fertility Society of Australia and New Zealand and a member of the Executive Board of the 'Doctors in ART' of the Fertility Society of Australia and New Zealand between 2019 and 2023. C.V. currently serves ESHRE as a Senior Deputy of the Steering Committee of the Special Interest Group Reproductive Endocrinology. He is also a fertility specialist offering his services to private patients. W.L. is a minority shareholder of CHA SMG Australia. R.J.N. declared research grant support from the Australian National Health and Medical Research Council for other projects, consulting or speaking fees from VinMec Vietnam, Westmead Fertility, Flinders Fertility, and Proadwise India, payment for lectures from Cadilla Pharma, and travel support from Merck Ltd L.R.J. declared research grant support from the Australian National Health and Medical Research Council for other projects. G.M.C. declared research grant support from the Australian National Health and Medical Research Council for other projects. G.M.C. is the Director of the National Perinatal Statistics and Epidemiology and Statistics Unit, UNSW, which prepares annual reports and benchmarking reports from the Australian and New Zealand Assisted Reproductive Technology Database (ANZARD). The remaining authors have no relevant disclosures for this study.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 2","pages":"hoaf020"},"PeriodicalIF":11.1000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12124915/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: Are the risks of adverse perinatal outcomes in singletons born from medically assisted reproduction (MAR) mainly associated with underlying parental infertility, or are they primarily linked to the MAR treatments?
Summary answer: While MAR-conceived singletons have increased risks of preterm birth, admission to neonatal intensive care unit (NICU), and hospital admission in early life, these risks are mainly associated with the underlying parental infertility that led to the use of MAR technologies.
What is known already: Children born from MAR are at increased risk for some adverse perinatal and infant outcomes. However, to what extent this risk is associated with infertility or MAR treatment remains unclear. This knowledge gap arises from the challenge in disentangling the effects of infertility and MAR treatment, given that parental infertility necessitates the use of MAR treatment.
Study design size duration: This is a statewide longitudinally data-linked population-based cohort study conducted in New South Wales, Australia, involving all singleton infants born (liveborn or stillborn) between 2009 and 2017.
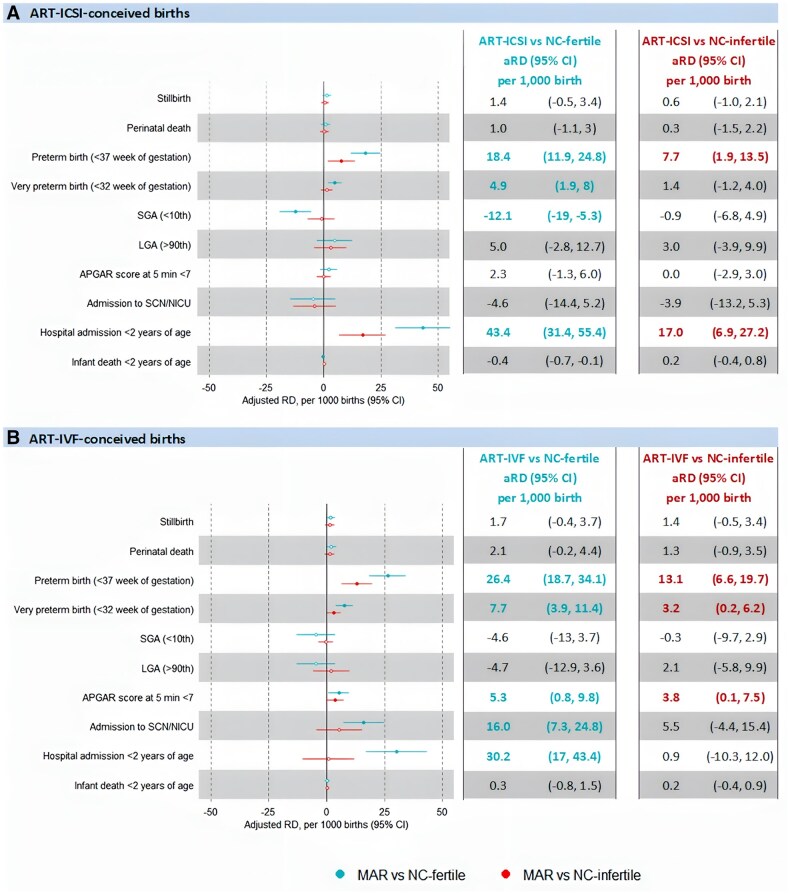
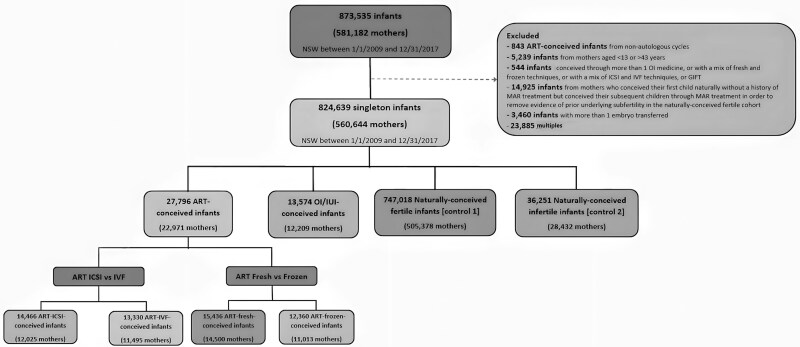
Participants/materials setting methods: We applied two comparisons to isolate the associations of infertility from its treatment: (i) MAR infants versus naturally conceived infants from fertile parents (NC-fertile), and (ii) MAR infants versus naturally conceived infants from parents who had a history of infertility (NC-infertile). The study cohort consisted of 824 639 singleton infants, of whom 27 796 (3.4%) were conceived through ART and 13 574 (1.6%) through ovulation induction/intrauterine insemination (OI/IUI), while 783 269 (95.0%) of the infants were naturally conceived (747 018 NC-fertile controls and 36 251 NC-infertile controls). We used the inverse probability of treatment weighting method to make MAR infants comparable with each of the two NC control groups. We then calculated the adjusted risk differences (aRDs) in these propensity score-weighted cohorts. In the subgroup analyses of different forms of ART treatment (ICSI vs IVF and fresh vs frozen embryo transfer), we reweighted the study cohort and compared these subgroups with the two NC control groups separately.
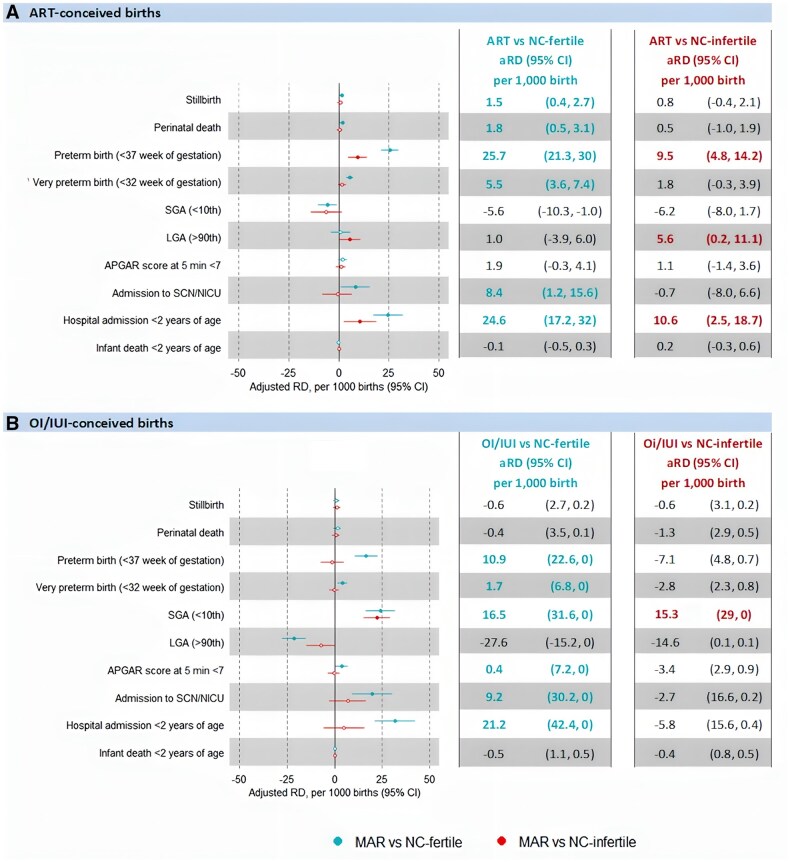
Main results and the role of chance: Singletons conceived through ART had a higher risk for preterm birth (aRD 25.7 per 1000 infants, 95% CI 21.3-30.0), admission to NICU (aRD 8.4 per 1000 infants, 95% CI 1.2-15.6), and hospital admission within 2 years of life (aRD 24.6 per 1000 infants, 95% CI 17.2-32.0) compared to NC-fertile controls. These risks were notably reduced when compared to NC-infertile controls (aRD 9.5 per 1000 infants, 95% CI 4.8-14.2 for preterm birth; -0.7 per 1000 infants, 95% CI -8.0 to 6.6 for NICU admission; and 10.6 per 1000 infants, 95% CI 2.5-18.7 for hospital admission within 2 years of life). ART-conceived singletons also had a higher risk of stillbirth compared to NC-fertile controls (aRD 1.5 per 1000 infants, 95% CI 0.4-2.7), which decreased when compared to NC-infertile controls (aRD 0.8 per 1000 infants, 95% CI -0.4 to 2.1). Similar patterns were observed for OI/IUI-conceived infants.Compared to NC-fertile controls, infants conceived by either ICSI (preterm birth: aRD 18.4 per 1000 infants, 95% CI 11.9-24.8; hospital admission: aRD 43.4 per 1000 infants, 95% CI 31.4-55.4) or IVF (preterm birth: aRD 26.4 per 1000 infants, 95% CI 18.7-34.1; hospital admission: aRD 30.2 per 1000 infants, 95% CI 17.0-43.4) had higher risks, but these risks decreased significantly when compared to NC-infertile controls (ICSI: preterm birth aRD 7.7 per 1000 infants, 95% CI 1.9-13.5; hospital admission aRD 17.0 per 1000 infants, 95% CI 6.9-27.2; IVF: preterm birth aRD 13.1 per 1000 infants, 95% CI 6.6-19.7; hospital admission aRD 0.9 per 1000 infants, 95% CI -10.3 to 12.0).Infants conceived by fresh ART transfers had higher risks of preterm birth (aRD 33.7 per 1000 infants, 95% CI 27.6-39.9) and hospital admission (aRD 33.7 per 1000 infants, 95% CI 23.5-43.9) compared to NC-fertile controls, with reduced risks when compared to NC-infertile controls (preterm birth: aRD 20.5 per 1000 infants, 95% CI 14.1-26.9; hospital admission: aRD 17.8 per 1000 infants, 95% CI 7.3-28.3). These risks were substantially lower for those conceived by frozen embryo transfers and came close to zero when compared to NC-infertile controls. However, frozen embryo transfer increased the risks of LGA (aRD 28.5 per 1000 infants, 95% CI 20.5-36.6) compared to NC-fertile controls, and this risk persisted when compared to NC-infertile controls.
Limitations reasons for caution: The observational nature and use of administrative data may carry a risk of misclassification or unmeasured confounding. We only included singletons because the risk profile for multiple births differs significantly. Parents with a history of infertility who achieved natural pregnancy likely had less severe conditions, potentially underestimating the contribution of parental infertility to perinatal risks.
Wider implications of the findings: The primary factor contributing to the increased risks of certain adverse perinatal outcomes is the underlying parental infertility that necessitates ART treatment. However, ART procedures also contribute to the risks to some extent; this study highlights the importance of careful monitoring and of reserving ART for where ART treatment is indicated.
Study funding/competing interests: This study is funded by the Australian National Health and Medical Research Council (APP1127437). The sponsors had no role in: the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. S.K.Y.C. is an employee of Sanofi, but this study was conducted before this role. W.L. declared research grant support from the Australian National Health and Medical Research Council for other projects. C.V. declared having received honoraria for invited lectures in scientific meetings/conferences, and/or having travel support, and/or being a member of advisory boards for Merck Ltd, Merck Sharpe & Dohme, Ferring, Organon, Vianex, Gedeon-Richter, and IBSA. C.V. was a minority shareholder of Virtus Health Ltd until June 2022 and a member of the Board of Directors of the Fertility Society of Australia and New Zealand and a member of the Executive Board of the 'Doctors in ART' of the Fertility Society of Australia and New Zealand between 2019 and 2023. C.V. currently serves ESHRE as a Senior Deputy of the Steering Committee of the Special Interest Group Reproductive Endocrinology. He is also a fertility specialist offering his services to private patients. W.L. is a minority shareholder of CHA SMG Australia. R.J.N. declared research grant support from the Australian National Health and Medical Research Council for other projects, consulting or speaking fees from VinMec Vietnam, Westmead Fertility, Flinders Fertility, and Proadwise India, payment for lectures from Cadilla Pharma, and travel support from Merck Ltd L.R.J. declared research grant support from the Australian National Health and Medical Research Council for other projects. G.M.C. declared research grant support from the Australian National Health and Medical Research Council for other projects. G.M.C. is the Director of the National Perinatal Statistics and Epidemiology and Statistics Unit, UNSW, which prepares annual reports and benchmarking reports from the Australian and New Zealand Assisted Reproductive Technology Database (ANZARD). The remaining authors have no relevant disclosures for this study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


