Tunnel combinations that should be avoided in anterior cruciate ligament reconstruction : a biomechanical assessment of 15 different combinations of femoral and tibial graft tunnels.
{"title":"Tunnel combinations that should be avoided in anterior cruciate ligament reconstruction : a biomechanical assessment of 15 different combinations of femoral and tibial graft tunnels.","authors":"Salameh Eljaja, Jørgen Tranum-Jensen, Mette Tavlo, Volkert Siersma, Michael Rindom Krogsgaard","doi":"10.1302/2633-1462.66.BJO-2025-0011.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Structured knowledge on the combined effect of various positions of femoral and tibial tunnels in reconstruction of the anterior cruciate ligament (ACL) on knee range of motion, rotatory stability, and anterior translatory laxity is limited. The aim was to test this for 15 regularly used tunnel combinations and identify combinations that should be avoided.</p><p><strong>Methods: </strong>A total of 60 cadaveric knees had the ACL removed and reconstructed. Flexion/extension, tibial rotation, and anterior tibial translation were measured with intact ACL, after ACL resection, and after ACL reconstructions with 15 tunnel combinations, based on five different femoral tunnels and three different tibial tunnels.</p><p><strong>Results: </strong>With a posterior tibial tunnel, the anterior tibial translation and tibial rotation increased when combined with most femoral tunnels. A transtibially positioned femoral tunnel when combined with any tibial tunnel caused flexion deficiency. Any femoral tunnel positioned by anteromedial technique combined with anterior or posterior tibia tunnels caused flexion deficiency. Severe extension deficiency was observed with an anterior tibial tunnel, in particular combined with a transtibially positioned femoral tunnel or an anterior femoral tunnel by anteromedial technique. Least anterior tibial translation combined with normal extension was achieved with a femoral tunnel by anteromedial technique as far posterior as possible, and an anatomically positioned tibial tunnel.</p><p><strong>Conclusion: </strong>In conclusion, tunnel combinations with the steepest (sagittal plane) and/or least oblique (frontal plane) grafts resulted in increased anterior tibial translation and tibial rotation, and should therefore be avoided. Anterior positioning of the graft caused extension deficiency, and there was flexion deficit with most grafts. A femoral tunnel as far posterior as possible by anteromedial technique is preferable in combination with an anatomically positioned tibial tunnel.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 6","pages":"618-625"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12127053/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.66.BJO-2025-0011.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Structured knowledge on the combined effect of various positions of femoral and tibial tunnels in reconstruction of the anterior cruciate ligament (ACL) on knee range of motion, rotatory stability, and anterior translatory laxity is limited. The aim was to test this for 15 regularly used tunnel combinations and identify combinations that should be avoided.
Methods: A total of 60 cadaveric knees had the ACL removed and reconstructed. Flexion/extension, tibial rotation, and anterior tibial translation were measured with intact ACL, after ACL resection, and after ACL reconstructions with 15 tunnel combinations, based on five different femoral tunnels and three different tibial tunnels.
Results: With a posterior tibial tunnel, the anterior tibial translation and tibial rotation increased when combined with most femoral tunnels. A transtibially positioned femoral tunnel when combined with any tibial tunnel caused flexion deficiency. Any femoral tunnel positioned by anteromedial technique combined with anterior or posterior tibia tunnels caused flexion deficiency. Severe extension deficiency was observed with an anterior tibial tunnel, in particular combined with a transtibially positioned femoral tunnel or an anterior femoral tunnel by anteromedial technique. Least anterior tibial translation combined with normal extension was achieved with a femoral tunnel by anteromedial technique as far posterior as possible, and an anatomically positioned tibial tunnel.
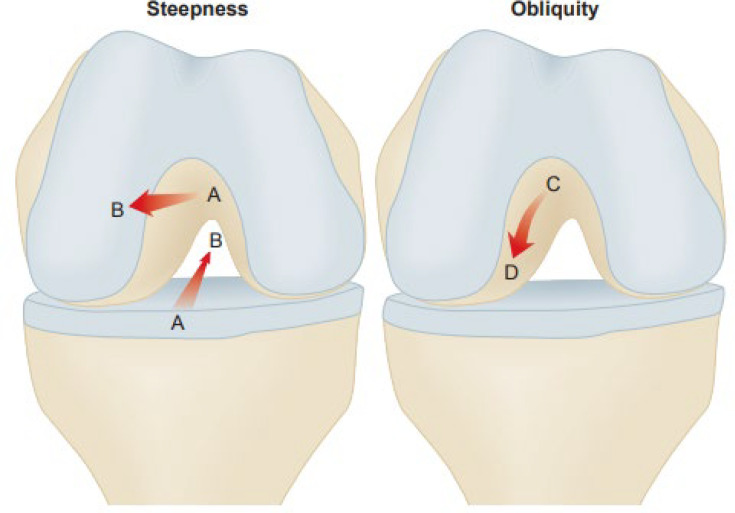
Conclusion: In conclusion, tunnel combinations with the steepest (sagittal plane) and/or least oblique (frontal plane) grafts resulted in increased anterior tibial translation and tibial rotation, and should therefore be avoided. Anterior positioning of the graft caused extension deficiency, and there was flexion deficit with most grafts. A femoral tunnel as far posterior as possible by anteromedial technique is preferable in combination with an anatomically positioned tibial tunnel.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


