Chau L B Ho, David Youens, Walter P Abhayaratna, Max K Bulsara, Jeff Hughes, Rachael Moorin, Sallie-Anne Pearson, David B Preen, Christopher M Reid, Rikje Ruiter, Christobel M Saunders, Bruno H Stricker, John Stubbs, Frank J A van Rooij, Cameron Wright, Ninh Thi Ha
{"title":"Estimation of the Duration of Antihypertensive Prescriptions: Validation of a Data-Driven Approach Using Rotterdam Study Data.","authors":"Chau L B Ho, David Youens, Walter P Abhayaratna, Max K Bulsara, Jeff Hughes, Rachael Moorin, Sallie-Anne Pearson, David B Preen, Christopher M Reid, Rikje Ruiter, Christobel M Saunders, Bruno H Stricker, John Stubbs, Frank J A van Rooij, Cameron Wright, Ninh Thi Ha","doi":"10.1002/pds.70164","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Administrative medicine dispensing data often omit prescribed duration, which is important for research on adherence or other pharmacoepidemiological topics. While the reverse waiting time distribution (rWTD) method has been widely used to estimate prescribed durations, its accuracy in real-world dispensing data is unknown. We assessed the performance of the rWTD method against the actual prescribed duration recorded in the Rotterdam Study.</p><p><strong>Methods: </strong>100 725 antihypertensive (AHT) prescriptions from 2018 to 2019 were extracted from the Rotterdam Study's medicine data. Data were constructed into five scenarios with increasing variability in the number of medicines included and variations in prescribed duration. The rWTD with 10 random index dates with or without adjustment for the quantity of dispensed medicine was conducted in all scenarios. Relative differences and limit of agreement ratio based on Bland-Altman analysis were used to examine agreement between estimated and actual prescribed durations.</p><p><strong>Results: </strong>rWTD models without adjustment for the quantity of dispensed medicine performed well only in the most homogenous scenario. In scenarios with greater data variability, performance improved significantly when adjusted for the quantity of dispensed medicine. Relative difference decreased from ≥ 65% in models without covariates to ≤ 20% with covariates, and the limit of agreement ratio decreased from ≥ 36.8 in models without covariates to ≤ 5.3 with covariates. Stratification analysis by subclass of the AHT medicines provided similar results.</p><p><strong>Conclusions: </strong>The study demonstrated that as data variability increased, the accuracy of the rWTD estimations decreased. However, the rWTD can produce good estimates (relative difference from 0% to 28%) of prescribed duration for AHT medicines, with the highest accuracy in the model adjusting for the quantity of dispensed medicine or stratification of the data with a relative difference less than 20% and the limit of agreement ratio less than 5.3 for the estimation at the 90th percentile of inter-arrival density. Since this validation was limited to antihypertensive medicines, generalizing the finding to other chronic-use medicines should be undertaken with caution.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 6","pages":"e70164"},"PeriodicalIF":2.4000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12127836/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70164","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Administrative medicine dispensing data often omit prescribed duration, which is important for research on adherence or other pharmacoepidemiological topics. While the reverse waiting time distribution (rWTD) method has been widely used to estimate prescribed durations, its accuracy in real-world dispensing data is unknown. We assessed the performance of the rWTD method against the actual prescribed duration recorded in the Rotterdam Study.
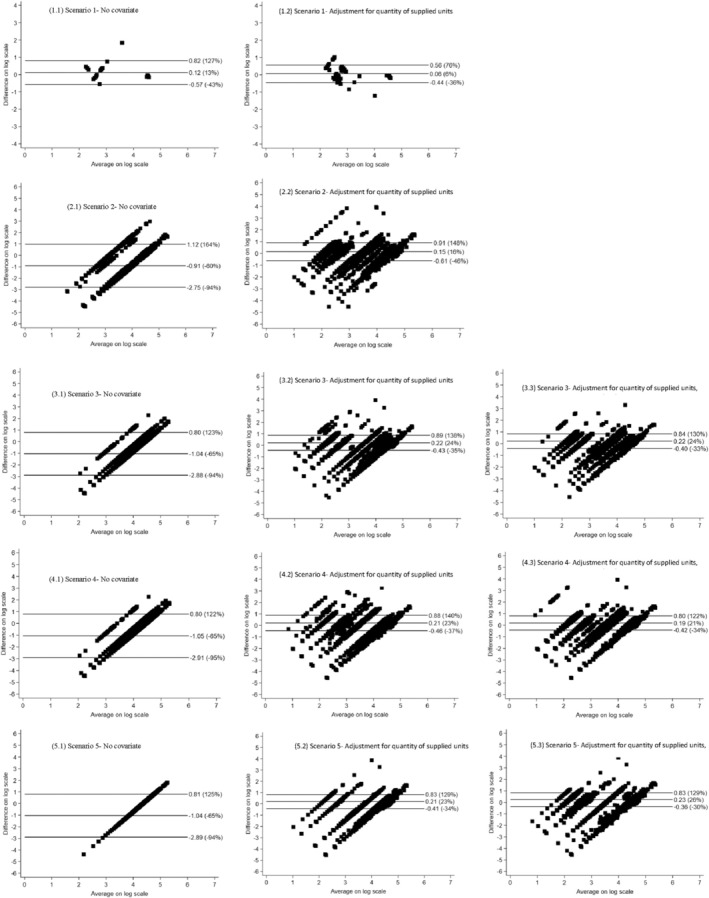
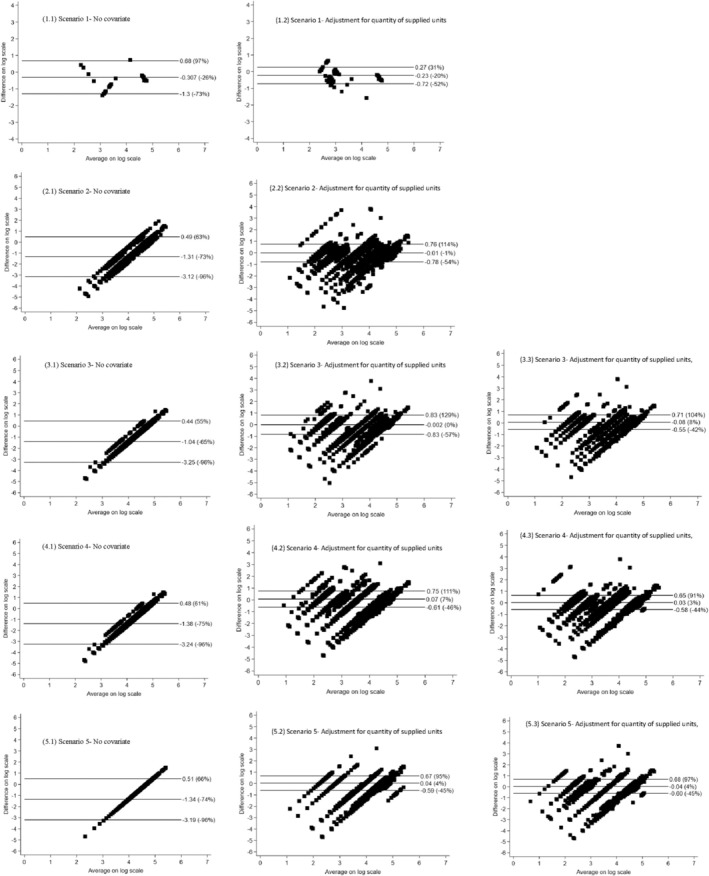
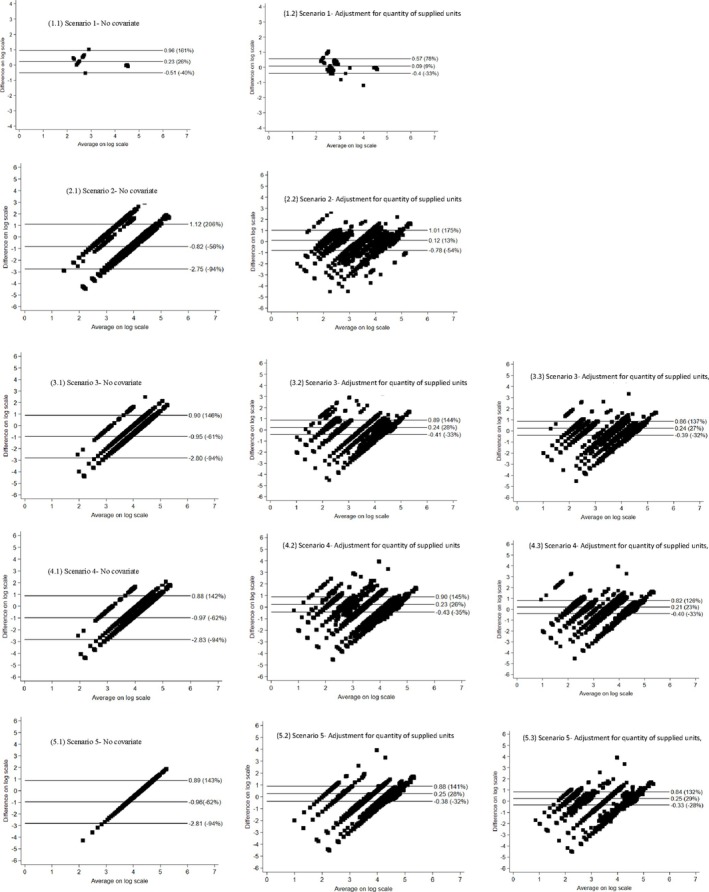
Methods: 100 725 antihypertensive (AHT) prescriptions from 2018 to 2019 were extracted from the Rotterdam Study's medicine data. Data were constructed into five scenarios with increasing variability in the number of medicines included and variations in prescribed duration. The rWTD with 10 random index dates with or without adjustment for the quantity of dispensed medicine was conducted in all scenarios. Relative differences and limit of agreement ratio based on Bland-Altman analysis were used to examine agreement between estimated and actual prescribed durations.
Results: rWTD models without adjustment for the quantity of dispensed medicine performed well only in the most homogenous scenario. In scenarios with greater data variability, performance improved significantly when adjusted for the quantity of dispensed medicine. Relative difference decreased from ≥ 65% in models without covariates to ≤ 20% with covariates, and the limit of agreement ratio decreased from ≥ 36.8 in models without covariates to ≤ 5.3 with covariates. Stratification analysis by subclass of the AHT medicines provided similar results.
Conclusions: The study demonstrated that as data variability increased, the accuracy of the rWTD estimations decreased. However, the rWTD can produce good estimates (relative difference from 0% to 28%) of prescribed duration for AHT medicines, with the highest accuracy in the model adjusting for the quantity of dispensed medicine or stratification of the data with a relative difference less than 20% and the limit of agreement ratio less than 5.3 for the estimation at the 90th percentile of inter-arrival density. Since this validation was limited to antihypertensive medicines, generalizing the finding to other chronic-use medicines should be undertaken with caution.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


