Associations between preoperative opioids, posthospitalization discharge disposition, and long-term opioid prescribing after spine surgery: a population-based cohort study.
Savannah Rose Whitfield, Andrew Charles Hanson, Erica Bellamkonda, Maria Mendoza De La Garza, Xander Schmidt, William Michael Hooten, Nafisseh Sirjani Warner
{"title":"Associations between preoperative opioids, posthospitalization discharge disposition, and long-term opioid prescribing after spine surgery: a population-based cohort study.","authors":"Savannah Rose Whitfield, Andrew Charles Hanson, Erica Bellamkonda, Maria Mendoza De La Garza, Xander Schmidt, William Michael Hooten, Nafisseh Sirjani Warner","doi":"10.31616/asj.2024.0414","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A retrospective cohort study.</p><p><strong>Purpose: </strong>To evaluate the association between preoperative opioid use and discharge disposition following major spine surgery and between discharge disposition and opioid availability through 1 year postoperatively.</p><p><strong>Overview of literature: </strong>Preoperative opioid use is prevalent in spine surgery and is associated with larger postoperative opioid consumption, longer hospitalizations, increased healthcare expenses, and greater risk of surgical revision. However, whether preoperative opioid use is associated with discharge disposition following major spine surgery, which may serve as an indicator of postoperative functional recovery, remains unclear.</p><p><strong>Methods: </strong>This retrospective population-based cohort study incorporated comprehensive prescription opioid information for 2223 adults (age ≥18 years) undergoing spine surgery in Olmsted County, Minnesota, between January 1, 2005, and December 31, 2016. Multivariable models were employed to assess the relationships among preoperative opioid exposures, postoperative opioid exposures, and discharge disposition (home, inpatient rehabilitation facility [IRF], and skilled nursing facility [SNF]).</p><p><strong>Results: </strong>A total of 2,223 adults were included with the following preoperative opioid availability: none (778 [35.0%]), short term (1,118 [50.3%]), episodic (227 [10.2%]), and long term (100 [4.5%]). Discharge dispositions were home (1,984 [89.2%]), IRF (94 [4.2%]), and SNF (145 [6.5%]). Compared with patients with no preoperative opioid availability, those with short-term or episodic opioid availability are less likely to be discharged to an IRF (odds ratio [OR], 0.56; 95% confidence interval [CI], 0.36-0.87; p=0.010). Patients with long-term opioid availability had significantly increased odds of SNF discharge (OR, 2.93; 95% CI, 1.39-6.17; p=0.005). At 1-year follow-up, patients discharged to IRF had an increased likelihood of long-term postoperative opioid availability compared with those discharged home (OR, 12.49; 95% CI, 4.84-32.24; p<0.001).</p><p><strong>Conclusions: </strong>Preoperative opioid prescribing was associated with post-hospitalization discharge disposition, which in turn was associated with opioid prescribing patterns 1 year postoperatively. Assessing opioid prescribing trends preoperatively may guide discussions regarding anticipated discharge disposition following spine surgery.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"590-599"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400098/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0414","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: A retrospective cohort study.
Purpose: To evaluate the association between preoperative opioid use and discharge disposition following major spine surgery and between discharge disposition and opioid availability through 1 year postoperatively.
Overview of literature: Preoperative opioid use is prevalent in spine surgery and is associated with larger postoperative opioid consumption, longer hospitalizations, increased healthcare expenses, and greater risk of surgical revision. However, whether preoperative opioid use is associated with discharge disposition following major spine surgery, which may serve as an indicator of postoperative functional recovery, remains unclear.
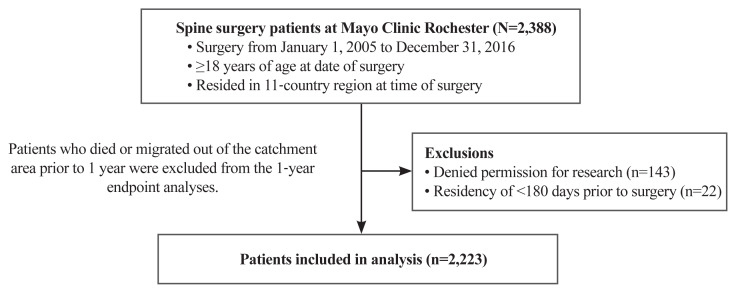
Methods: This retrospective population-based cohort study incorporated comprehensive prescription opioid information for 2223 adults (age ≥18 years) undergoing spine surgery in Olmsted County, Minnesota, between January 1, 2005, and December 31, 2016. Multivariable models were employed to assess the relationships among preoperative opioid exposures, postoperative opioid exposures, and discharge disposition (home, inpatient rehabilitation facility [IRF], and skilled nursing facility [SNF]).
Results: A total of 2,223 adults were included with the following preoperative opioid availability: none (778 [35.0%]), short term (1,118 [50.3%]), episodic (227 [10.2%]), and long term (100 [4.5%]). Discharge dispositions were home (1,984 [89.2%]), IRF (94 [4.2%]), and SNF (145 [6.5%]). Compared with patients with no preoperative opioid availability, those with short-term or episodic opioid availability are less likely to be discharged to an IRF (odds ratio [OR], 0.56; 95% confidence interval [CI], 0.36-0.87; p=0.010). Patients with long-term opioid availability had significantly increased odds of SNF discharge (OR, 2.93; 95% CI, 1.39-6.17; p=0.005). At 1-year follow-up, patients discharged to IRF had an increased likelihood of long-term postoperative opioid availability compared with those discharged home (OR, 12.49; 95% CI, 4.84-32.24; p<0.001).
Conclusions: Preoperative opioid prescribing was associated with post-hospitalization discharge disposition, which in turn was associated with opioid prescribing patterns 1 year postoperatively. Assessing opioid prescribing trends preoperatively may guide discussions regarding anticipated discharge disposition following spine surgery.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


