Milene Rangel da Costa, Bráulio Dos Santos Júnior, Marisa da Silva Santos
{"title":"Adjusting Health State Utility Values for Multiple Conditions: Real-World EQ-5D-3L Data Modeling in Brazil.","authors":"Milene Rangel da Costa, Bráulio Dos Santos Júnior, Marisa da Silva Santos","doi":"10.1007/s41669-025-00586-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Decision analytical models are typically included in health economic evaluations to represent clinical pathways and enable the estimation of clinical and economic outcomes of health technologies. Clinical effects are frequently measured in terms of health-related quality of life and expressed as utility values. It is not rare that a health state in an analytical model simultaneously comprises more than one health condition. In this situation, the utility of each coexisting health condition could be combined using the additive, multiplicative, minimum, or adjusted decrement estimator (ADE) methods. However, there is no consensus about the best approach. This study aimed to compare different methods to estimate utility values for health states in which patients carry more than one health condition using data from the Brazilian population.</p><p><strong>Methods: </strong>Data were obtained from a multicentric cross-sectional evaluation study conducted in Brazil. Individuals completed the EQ-5D-3L questionnaire, a generic preference-based instrument that is used to obtain utility values, and were requested to disclose if they had any health conditions. Utilities were obtained according to the Brazilian value set. Four methods for adjusting joint utilities were tested: additive, multiplicative, minimum, and ADE. Observed and estimated utility values were compared for accuracy and bias.</p><p><strong>Results: </strong>A total of 5774 individuals were included in the analysis. The utility score (mean ± SE) was 0.8235 ± 0.1717. Lower utility scores were associated with an increased number of comorbidities, reaching 0.467 ± 0.192 for individuals with seven conditions. The minimum method produced accurate utility estimates for individuals with two simultaneous health conditions. For health states with more than two conditions, the multiplicative method presented more accurate estimates. Overall, fixing the baseline utility equal to the mean utility of healthy individuals produced less biased estimates compared with a baseline utility equal to 1.</p><p><strong>Conclusion: </strong>Depending on the utility data available and the number of concomitant conditions, different adjustment methods could be used that produce accurate estimates. For the adjustment of Brazilian utility values for health states with comorbidities, the minimum and multiplicative methods should be preferred if two or more than two conditions are present, respectively.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"785-791"},"PeriodicalIF":2.1000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00586-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/31 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Decision analytical models are typically included in health economic evaluations to represent clinical pathways and enable the estimation of clinical and economic outcomes of health technologies. Clinical effects are frequently measured in terms of health-related quality of life and expressed as utility values. It is not rare that a health state in an analytical model simultaneously comprises more than one health condition. In this situation, the utility of each coexisting health condition could be combined using the additive, multiplicative, minimum, or adjusted decrement estimator (ADE) methods. However, there is no consensus about the best approach. This study aimed to compare different methods to estimate utility values for health states in which patients carry more than one health condition using data from the Brazilian population.
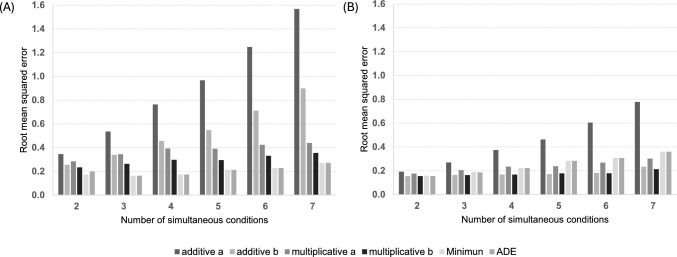
Methods: Data were obtained from a multicentric cross-sectional evaluation study conducted in Brazil. Individuals completed the EQ-5D-3L questionnaire, a generic preference-based instrument that is used to obtain utility values, and were requested to disclose if they had any health conditions. Utilities were obtained according to the Brazilian value set. Four methods for adjusting joint utilities were tested: additive, multiplicative, minimum, and ADE. Observed and estimated utility values were compared for accuracy and bias.
Results: A total of 5774 individuals were included in the analysis. The utility score (mean ± SE) was 0.8235 ± 0.1717. Lower utility scores were associated with an increased number of comorbidities, reaching 0.467 ± 0.192 for individuals with seven conditions. The minimum method produced accurate utility estimates for individuals with two simultaneous health conditions. For health states with more than two conditions, the multiplicative method presented more accurate estimates. Overall, fixing the baseline utility equal to the mean utility of healthy individuals produced less biased estimates compared with a baseline utility equal to 1.
Conclusion: Depending on the utility data available and the number of concomitant conditions, different adjustment methods could be used that produce accurate estimates. For the adjustment of Brazilian utility values for health states with comorbidities, the minimum and multiplicative methods should be preferred if two or more than two conditions are present, respectively.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


