Yub Raj Sedhai, Priyanka Bhat, Roshan Acharya, Nada Qaiser Qureshi, Fawaz Mohammed, Irfan Waheed, Tahir Muhammad Abdullah Khan, Muhammad Altaf Ahmed, Nisarfathima Kazimuddin, Akinchan Kafle, Rodney T Steff, Karan Singh
{"title":"Intrapleural tissue plasminogen activator and deoxyribonuclease in complex pleural effusion and empyema, clinical outcomes, and predictors.","authors":"Yub Raj Sedhai, Priyanka Bhat, Roshan Acharya, Nada Qaiser Qureshi, Fawaz Mohammed, Irfan Waheed, Tahir Muhammad Abdullah Khan, Muhammad Altaf Ahmed, Nisarfathima Kazimuddin, Akinchan Kafle, Rodney T Steff, Karan Singh","doi":"10.1177/17534666251343711","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Complex pleural effusion and empyema (CPPE) is treated with intrapleural fibrinolytic therapy (IPFT) using tissue plasminogen activator (tPA) and deoxyribonuclease (DNase) We present our single-center retrospective observational data using a simplified regimen of coadministering six divided doses of tPA and DNase over the course of 3 days.</p><p><strong>Objective: </strong>To study the safety, utility, and clinical outcomes of IPFT.</p><p><strong>Design: </strong>This is a single-center retrospective study of patients who received co-administration tPA/DNase for CPPE over a period of 5 years. The primary outcome was successful treatment without the need for surgery. Secondary outcomes were bleeding risk, post-procedural pain, treatment complications, and all-cause mortality at 30 days and 6 months. We have tested the clinical role RAPID score (Renal function measured as urea, Age, fluid Purulence, Infection source, Dietary status measured as albumin) to predict treatment success, and all-cause mortality at 6 months.</p><p><strong>Results: </strong>A total of (<i>n</i> = 55) patients were included in the study. The mean age of the population studied was 67 (Interquartile range 57-74), including 47.3% male and 52.7% Female. 92.7% of the population studied was Caucasian. Comorbidities including chronic obstructive pulmonary disease, congestive heart failure, and Diabetes mellitus were present in 41.8%, 41.8%, and 43.6.% respectively. Patients were treated with tube thoracostomy with 14 French percutaneous pigtail catheters in 47 (85.5%) or 28-32 French chest tubes in 8 (14.5%) patients. Twenty-nine percent (16) of patients had acceptable clinical and radiographic improvement and did not require additional surgical or radiological intervention. Seventy-one percent (39) of patients required additional surgical drainage; video-assisted thoracoscopic surgery in 37, and open thoracotomy in 2 patients. The discriminating ability of the RAPID score for treatment success after IPFT was found to be poor (AUC: 0.601, 95% CI: 0.429-0.773, <i>p</i> = 0.24). All-cause mortality at 6 months was 23.6% (13) of patients. The predictive ability of the RAPID score for mortality at 6 months was found to be poor (AUC: 0.640, 95% CI: 0.478-0.802, <i>p</i> = 0.13). The optimal cutoff for the RAPID score for mortality was ⩾4, with 84.6% sensitivity and 46.3% specificity.</p><p><strong>Conclusion: </strong>Results of our single-center study suggest that IPFT can be safely adopted by small and mid-sized clinical centers, as the risk of bleeding is low. The results of coadministering tPA and DNase are safe, and it reduces the need for surgical intervention in nearly one-third of patients.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"19 ","pages":"17534666251343711"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126679/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666251343711","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
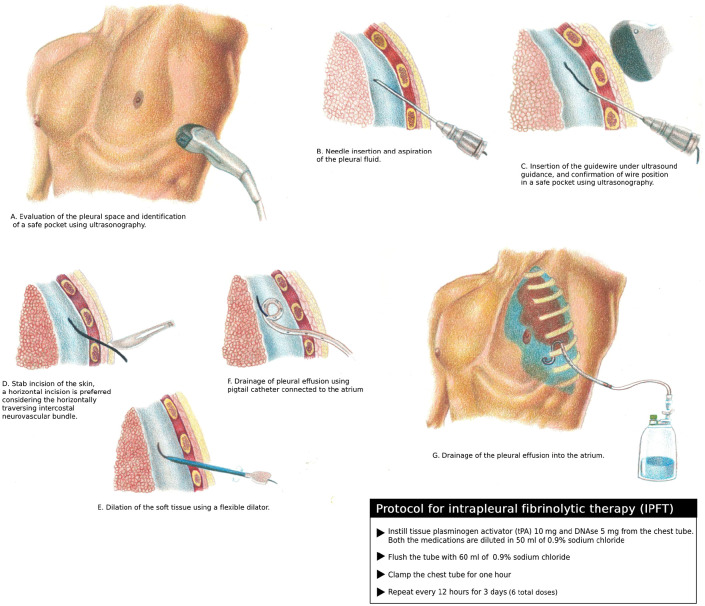
Background: Complex pleural effusion and empyema (CPPE) is treated with intrapleural fibrinolytic therapy (IPFT) using tissue plasminogen activator (tPA) and deoxyribonuclease (DNase) We present our single-center retrospective observational data using a simplified regimen of coadministering six divided doses of tPA and DNase over the course of 3 days.
Objective: To study the safety, utility, and clinical outcomes of IPFT.
Design: This is a single-center retrospective study of patients who received co-administration tPA/DNase for CPPE over a period of 5 years. The primary outcome was successful treatment without the need for surgery. Secondary outcomes were bleeding risk, post-procedural pain, treatment complications, and all-cause mortality at 30 days and 6 months. We have tested the clinical role RAPID score (Renal function measured as urea, Age, fluid Purulence, Infection source, Dietary status measured as albumin) to predict treatment success, and all-cause mortality at 6 months.
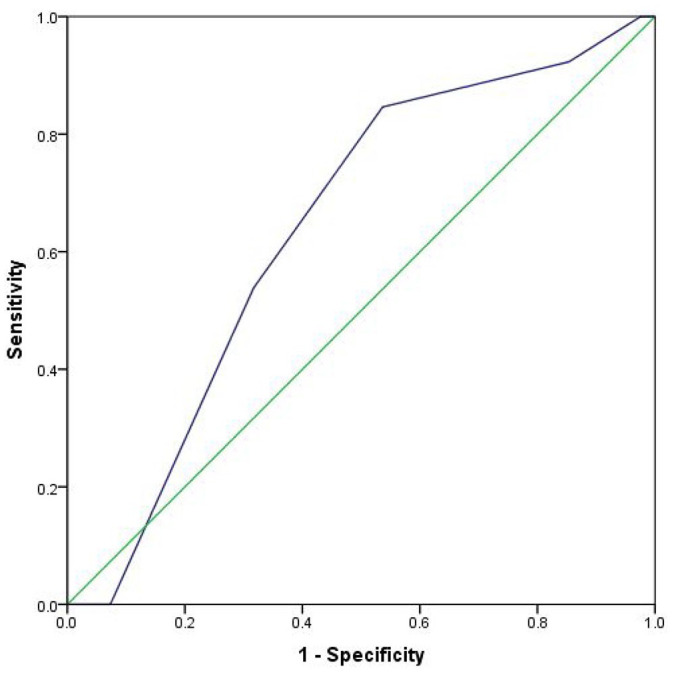
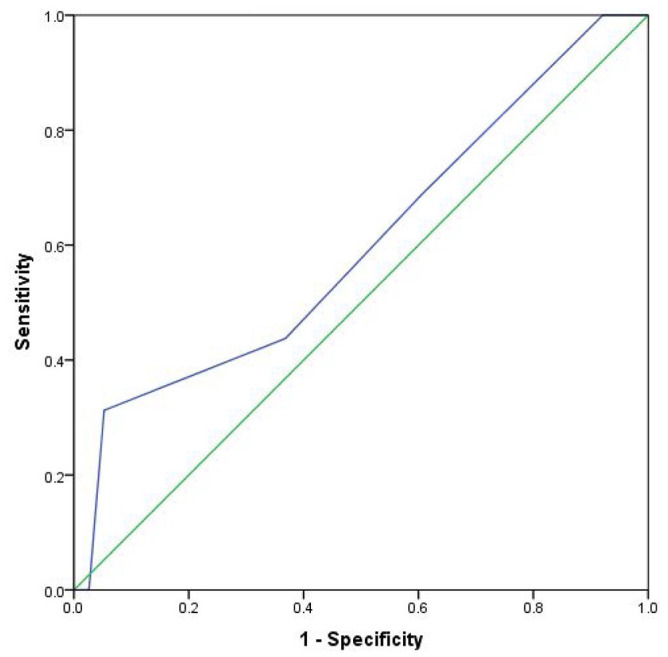
Results: A total of (n = 55) patients were included in the study. The mean age of the population studied was 67 (Interquartile range 57-74), including 47.3% male and 52.7% Female. 92.7% of the population studied was Caucasian. Comorbidities including chronic obstructive pulmonary disease, congestive heart failure, and Diabetes mellitus were present in 41.8%, 41.8%, and 43.6.% respectively. Patients were treated with tube thoracostomy with 14 French percutaneous pigtail catheters in 47 (85.5%) or 28-32 French chest tubes in 8 (14.5%) patients. Twenty-nine percent (16) of patients had acceptable clinical and radiographic improvement and did not require additional surgical or radiological intervention. Seventy-one percent (39) of patients required additional surgical drainage; video-assisted thoracoscopic surgery in 37, and open thoracotomy in 2 patients. The discriminating ability of the RAPID score for treatment success after IPFT was found to be poor (AUC: 0.601, 95% CI: 0.429-0.773, p = 0.24). All-cause mortality at 6 months was 23.6% (13) of patients. The predictive ability of the RAPID score for mortality at 6 months was found to be poor (AUC: 0.640, 95% CI: 0.478-0.802, p = 0.13). The optimal cutoff for the RAPID score for mortality was ⩾4, with 84.6% sensitivity and 46.3% specificity.
Conclusion: Results of our single-center study suggest that IPFT can be safely adopted by small and mid-sized clinical centers, as the risk of bleeding is low. The results of coadministering tPA and DNase are safe, and it reduces the need for surgical intervention in nearly one-third of patients.
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


