Cost-effective pricing of long-acting injectable HIV pre-exposure prophylaxis for adolescent girls and young women in South Africa: a model-based analysis.
IF 19.9 1区 医学Q1 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Elena Y Jin, Ali R Ahmed, Linda-Gail Bekker, Elzette Rousseau, Caitlin M Dugdale, Clare F Flanagan, Melissa Wallace, Kenneth A Freedberg, Catherine Orrell, Krishna P Reddy, A David Paltiel, Andrea L Ciaranello, Anne M Neilan
{"title":"Cost-effective pricing of long-acting injectable HIV pre-exposure prophylaxis for adolescent girls and young women in South Africa: a model-based analysis.","authors":"Elena Y Jin, Ali R Ahmed, Linda-Gail Bekker, Elzette Rousseau, Caitlin M Dugdale, Clare F Flanagan, Melissa Wallace, Kenneth A Freedberg, Catherine Orrell, Krishna P Reddy, A David Paltiel, Andrea L Ciaranello, Anne M Neilan","doi":"10.1016/S2214-109X(25)00119-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Long-acting, injectable cabotegravir (CAB-LA) is more effective than daily oral tenofovir disoproxil fumarate and emtricitabine (TDF-FTC) for HIV pre-exposure prophylaxis (PrEP). We aimed to estimate the maximum price premium: the greatest price markup that society should be willing to accept for CAB-LA compared with TDF-FTC among adolescent girls and young women aged 15-29 years in South Africa.</p><p><strong>Methods: </strong>Using the Cost-effectiveness of Preventing AIDS Complications model, we simulated adolescent girls and young women (aged 15-29 years) with characteristics similar to the targeted enrolment population of the FastPrEP study in Cape Town, South Africa, to compare daily oral TDF-FTC with bimonthly CAB-LA. The simulation model captured individual and population-level effects from a health-care sector perspective. Model inputs included HIV incidence (off PrEP 3·2 per 100 person-years, TDF-FTC 1·9 per 100 person-years, and CAB-LA 0·2 per 100 person-years), 10-year cumulative HIV transmissions to partners, and PrEP persistence (TDF-FTC 88% and CAB-LA 85% at 2 years) from published data. Annual costs included PrEP programme (TDF-FTC US$28 and CAB-LA $45), PrEP drug (TDF-FTC $40), antiretroviral therapy ($50-890), and HIV-related care ($230-1800). Model-projected outcomes included incident infections among adolescent girls and young women, transmissions, life-years, costs, incremental cost-effectiveness ratios (ICERs), and the maximum price premium of CAB-LA drug at a willingness-to-pay threshold of 50% of the gross domestic product of South Africa per capita ($3500 per life-year). Key parameters were varied in sensitivity analyses.</p><p><strong>Findings: </strong>Per 10 000 adolescent girls and young women and their partners over 10 years, our model estimates that infections and transmissions would be higher, and life-years would be lower using a TDF-FTC strategy (1980 infections, 450 transmissions, and 88 400 life-years) compared with CAB-LA (1080 infections, 220 transmission, and 88 600 discounted life-years). At 10 years, CAB-LA would be cost-effective with a maximum price premium over TDF-FTC of $38 per year (maximum price of $78 per year) and cost-saving at a drug price of $65 per year. Considering a lifetime horizon, the maximum price premium over TDF-FTC could be seven times higher: $232 per year (maximum price $272 per year).</p><p><strong>Interpretation: </strong>Our findings suggest that a CAB-LA strategy could reduce transmissions and increase life-years compared with TDF-FTC. The availability of an inexpensive and effective oral alternative medication for adolescent girls and young women in South Africa limits the price that payers should be willing to accept for CAB-LA with a modest markup over TDF-FTC.</p><p><strong>Funding: </strong>National Institutes of Health and Massachusetts General Hospital Executive Committee on Research.</p>","PeriodicalId":48783,"journal":{"name":"Lancet Global Health","volume":" ","pages":"e1230-e1239"},"PeriodicalIF":19.9000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12223965/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lancet Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/S2214-109X(25)00119-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Long-acting, injectable cabotegravir (CAB-LA) is more effective than daily oral tenofovir disoproxil fumarate and emtricitabine (TDF-FTC) for HIV pre-exposure prophylaxis (PrEP). We aimed to estimate the maximum price premium: the greatest price markup that society should be willing to accept for CAB-LA compared with TDF-FTC among adolescent girls and young women aged 15-29 years in South Africa.
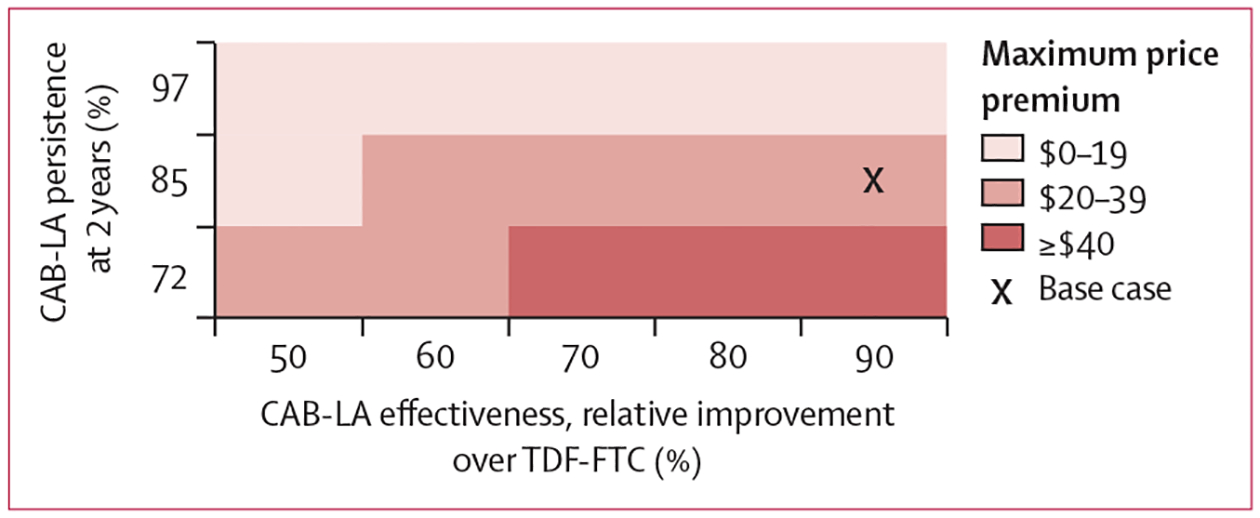
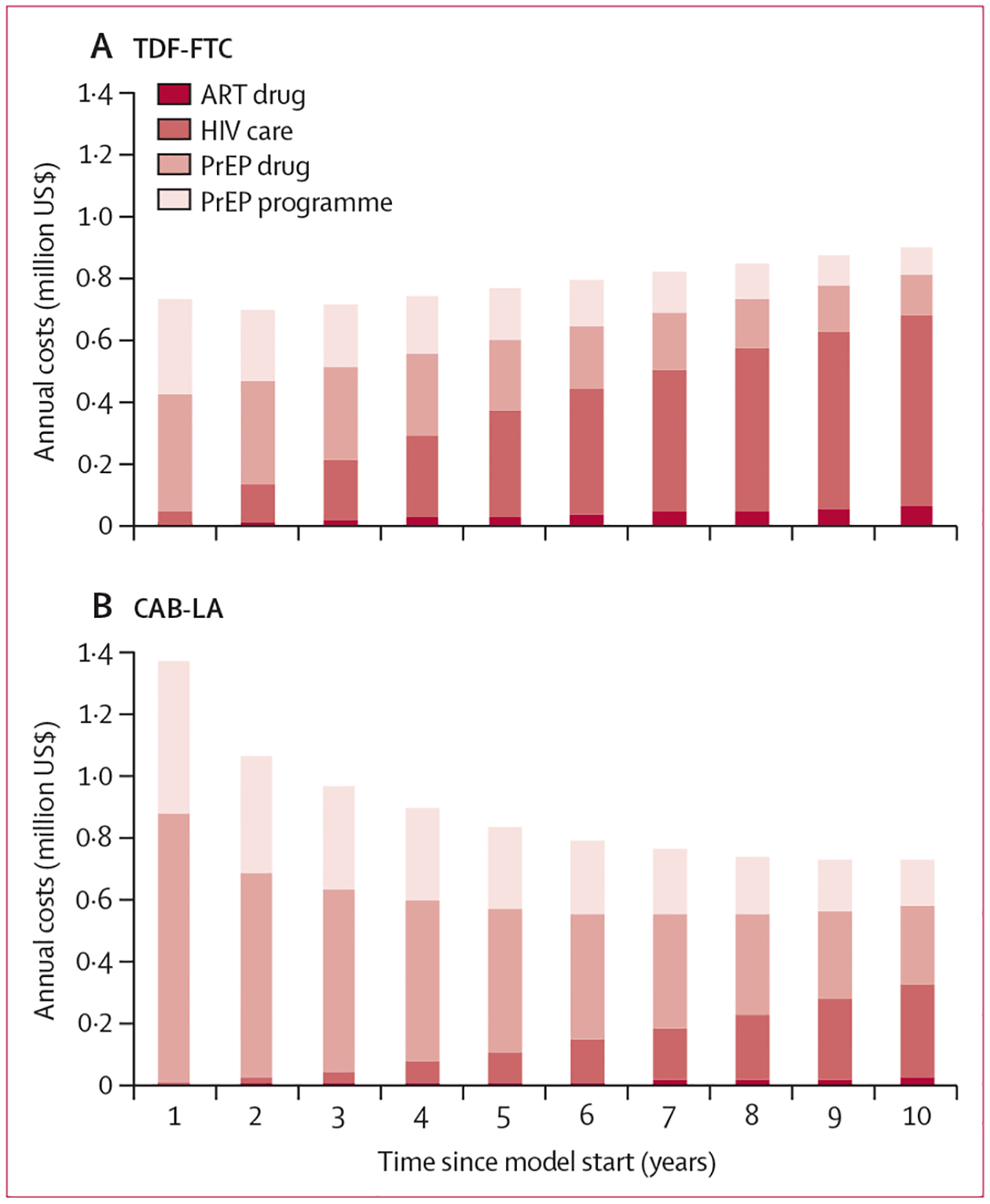
Methods: Using the Cost-effectiveness of Preventing AIDS Complications model, we simulated adolescent girls and young women (aged 15-29 years) with characteristics similar to the targeted enrolment population of the FastPrEP study in Cape Town, South Africa, to compare daily oral TDF-FTC with bimonthly CAB-LA. The simulation model captured individual and population-level effects from a health-care sector perspective. Model inputs included HIV incidence (off PrEP 3·2 per 100 person-years, TDF-FTC 1·9 per 100 person-years, and CAB-LA 0·2 per 100 person-years), 10-year cumulative HIV transmissions to partners, and PrEP persistence (TDF-FTC 88% and CAB-LA 85% at 2 years) from published data. Annual costs included PrEP programme (TDF-FTC US$28 and CAB-LA $45), PrEP drug (TDF-FTC $40), antiretroviral therapy ($50-890), and HIV-related care ($230-1800). Model-projected outcomes included incident infections among adolescent girls and young women, transmissions, life-years, costs, incremental cost-effectiveness ratios (ICERs), and the maximum price premium of CAB-LA drug at a willingness-to-pay threshold of 50% of the gross domestic product of South Africa per capita ($3500 per life-year). Key parameters were varied in sensitivity analyses.
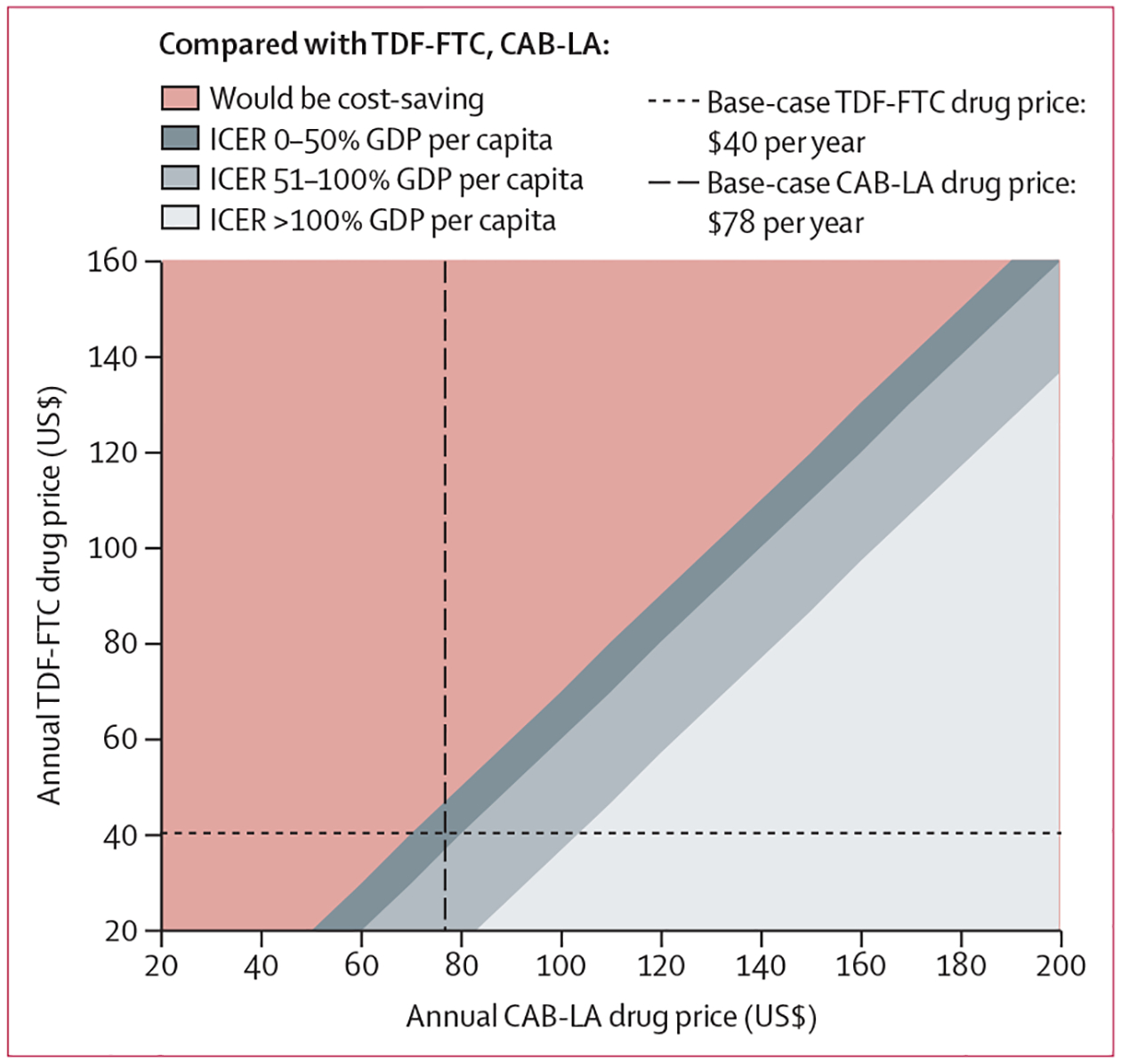
Findings: Per 10 000 adolescent girls and young women and their partners over 10 years, our model estimates that infections and transmissions would be higher, and life-years would be lower using a TDF-FTC strategy (1980 infections, 450 transmissions, and 88 400 life-years) compared with CAB-LA (1080 infections, 220 transmission, and 88 600 discounted life-years). At 10 years, CAB-LA would be cost-effective with a maximum price premium over TDF-FTC of $38 per year (maximum price of $78 per year) and cost-saving at a drug price of $65 per year. Considering a lifetime horizon, the maximum price premium over TDF-FTC could be seven times higher: $232 per year (maximum price $272 per year).
Interpretation: Our findings suggest that a CAB-LA strategy could reduce transmissions and increase life-years compared with TDF-FTC. The availability of an inexpensive and effective oral alternative medication for adolescent girls and young women in South Africa limits the price that payers should be willing to accept for CAB-LA with a modest markup over TDF-FTC.
Funding: National Institutes of Health and Massachusetts General Hospital Executive Committee on Research.
期刊介绍:
The Lancet Global Health is an online publication that releases monthly open access (subscription-free) issues.Each issue includes original research, commentary, and correspondence.In addition to this, the publication also provides regular blog posts.
The main focus of The Lancet Global Health is on disadvantaged populations, which can include both entire economic regions and marginalized groups within prosperous nations.The publication prefers to cover topics related to reproductive, maternal, neonatal, child, and adolescent health; infectious diseases (including neglected tropical diseases); non-communicable diseases; mental health; the global health workforce; health systems; surgery; and health policy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


