Komal Abdul Rahim, Namra Qadeer Shaikh, Maryam Pyar Ali Lakhdir, Asma Altaf Hussain Merchant, Noreen Afzal, Saad Bin Zafar Mahmood, Saqib Kamran Bakhshi, Mushyada Ali, Zainab Samad, Adil H Haider
{"title":"Identifying those at risk: predicting patient factors associated with worse EGS outcomes.","authors":"Komal Abdul Rahim, Namra Qadeer Shaikh, Maryam Pyar Ali Lakhdir, Asma Altaf Hussain Merchant, Noreen Afzal, Saad Bin Zafar Mahmood, Saqib Kamran Bakhshi, Mushyada Ali, Zainab Samad, Adil H Haider","doi":"10.1136/tsaco-2024-001690","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Comorbidity has a detrimental impact on Emergency General Surgery (EGS) outcomes. In lesser-developed countries with inconsistent documentation of comorbid conditions, undiagnosed and progressively worsening comorbidities can worsen EGS outcomes. We aimed to discern the comorbidity index as a predictor of complications and inpatient mortality in EGS using a large South Asian sample population.</p><p><strong>Materials and methods: </strong>Data of adult patients with AAST-defined EGS diagnoses at primary index admission from 2010 to 2019 were retrieved. Patients were categorized into predefined EGS groups using ICD-9 CM codes. Primary exposure was comorbidity using the Charlson Comorbidity Index (CCI). The primary outcome was inpatient mortality, and the secondary outcome was complication status. Multiple logistic and Cox regression with Weibull distribution was performed.</p><p><strong>Results: </strong>Analysis of 32 280 patients showed a mean age of 40.06±16.87 years. Overall comorbidity, inpatient mortality, and complication rates were 44.6%, 2.42% and 36.37%, respectively. Patients with moderate CCI had the highest complications (AOR 6.61, 95% CI 5.91, 7.37), and severe comorbidity had the highest hazards (AOR 3.79, 95% CI 2.89, 4.98). Male gender, increasing age, emergent admission status, and lack of insurance were associated with moderate and severe CCI, resulting in prolonged length of stay (5.72 and 5.83 days), reduced survival time (20.04 and 21.95 days), and higher mortality rates (10.52% and 9.48%).</p><p><strong>Conclusions: </strong>We identified predictive patient-level factors associated with higher CCI and worse EGS outcomes. Our findings can help stratify population subsets at risk of worse outcomes, provide valuable insight into disease progression, and aid decision-making in EGS patients.</p><p><strong>Level of evidence: </strong>III.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 2","pages":"e001690"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121602/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001690","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Comorbidity has a detrimental impact on Emergency General Surgery (EGS) outcomes. In lesser-developed countries with inconsistent documentation of comorbid conditions, undiagnosed and progressively worsening comorbidities can worsen EGS outcomes. We aimed to discern the comorbidity index as a predictor of complications and inpatient mortality in EGS using a large South Asian sample population.
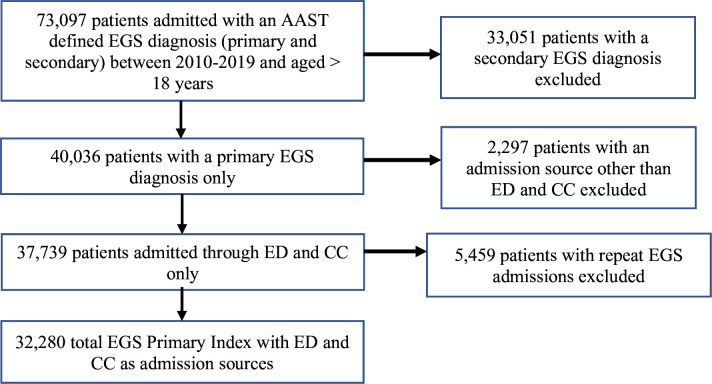
Materials and methods: Data of adult patients with AAST-defined EGS diagnoses at primary index admission from 2010 to 2019 were retrieved. Patients were categorized into predefined EGS groups using ICD-9 CM codes. Primary exposure was comorbidity using the Charlson Comorbidity Index (CCI). The primary outcome was inpatient mortality, and the secondary outcome was complication status. Multiple logistic and Cox regression with Weibull distribution was performed.
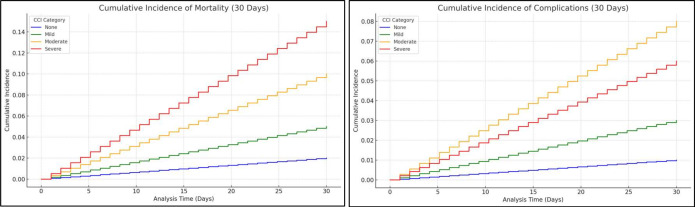
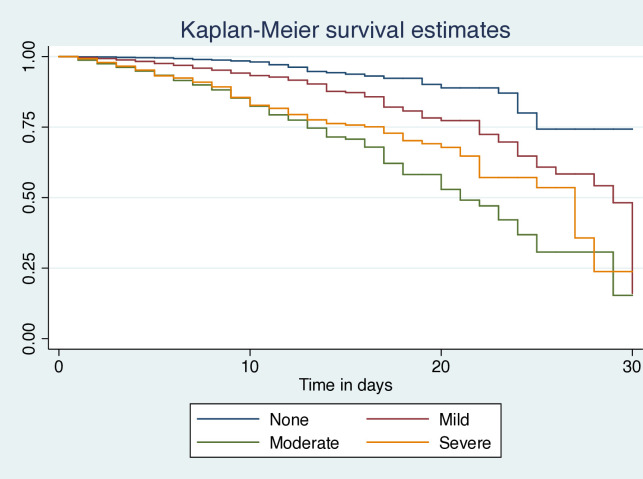
Results: Analysis of 32 280 patients showed a mean age of 40.06±16.87 years. Overall comorbidity, inpatient mortality, and complication rates were 44.6%, 2.42% and 36.37%, respectively. Patients with moderate CCI had the highest complications (AOR 6.61, 95% CI 5.91, 7.37), and severe comorbidity had the highest hazards (AOR 3.79, 95% CI 2.89, 4.98). Male gender, increasing age, emergent admission status, and lack of insurance were associated with moderate and severe CCI, resulting in prolonged length of stay (5.72 and 5.83 days), reduced survival time (20.04 and 21.95 days), and higher mortality rates (10.52% and 9.48%).
Conclusions: We identified predictive patient-level factors associated with higher CCI and worse EGS outcomes. Our findings can help stratify population subsets at risk of worse outcomes, provide valuable insight into disease progression, and aid decision-making in EGS patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


