Casper S Lansbergen, Rolf Fronczek, Leopoldine A Wilbrink, Steven P Cohen, Cecile C de Vos, Frank J P M Huygen
{"title":"15. Cluster Headache.","authors":"Casper S Lansbergen, Rolf Fronczek, Leopoldine A Wilbrink, Steven P Cohen, Cecile C de Vos, Frank J P M Huygen","doi":"10.1111/papr.70050","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cluster headache is a rare primary headache disorder characterized by excruciating unilateral pain around the eye, lasting between 15 and 180 min, accompanied by ipsilateral cranial autonomic symptoms. Cluster headache is classified into two forms: episodic and chronic, with chronic cluster headache defined by pain-free intervals of less than 3 months between bouts. Both drug-based and invasive treatments are available for abortive and preventive purposes. Treatment selection depends on individual efficacy and tolerance, with invasive options considered when pharmacological treatments prove ineffective.</p><p><strong>Methods: </strong>This narrative review summarizes the literature on common practice and the evidence in the treatment of cluster headache.</p><p><strong>Results: </strong>Oxygen therapy and subcutaneous sumatriptan are the most effective abortive treatments for cluster headache. Oral corticosteroid tapering regimens can be used as bridging therapy. Verapamil, lithium, topiramate, and CGRP antagonists are potential preventive medication options. Greater occipital nerve (GON) injections and radiofrequency (RF) therapy can be used as preventive treatments, though their effects are often temporary. For refractory chronic cluster headache, occipital nerve stimulation (ONS) has proven to be effective. Deep brain stimulation (DBS) may also be considered if all other treatments have failed.</p><p><strong>Conclusions: </strong>The management of cluster headache is complex due to the variable efficacy of treatments across different patients and limited evidence.</p>","PeriodicalId":19974,"journal":{"name":"Pain Practice","volume":"25 5","pages":"e70050"},"PeriodicalIF":2.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120220/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/papr.70050","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Cluster headache is a rare primary headache disorder characterized by excruciating unilateral pain around the eye, lasting between 15 and 180 min, accompanied by ipsilateral cranial autonomic symptoms. Cluster headache is classified into two forms: episodic and chronic, with chronic cluster headache defined by pain-free intervals of less than 3 months between bouts. Both drug-based and invasive treatments are available for abortive and preventive purposes. Treatment selection depends on individual efficacy and tolerance, with invasive options considered when pharmacological treatments prove ineffective.
Methods: This narrative review summarizes the literature on common practice and the evidence in the treatment of cluster headache.
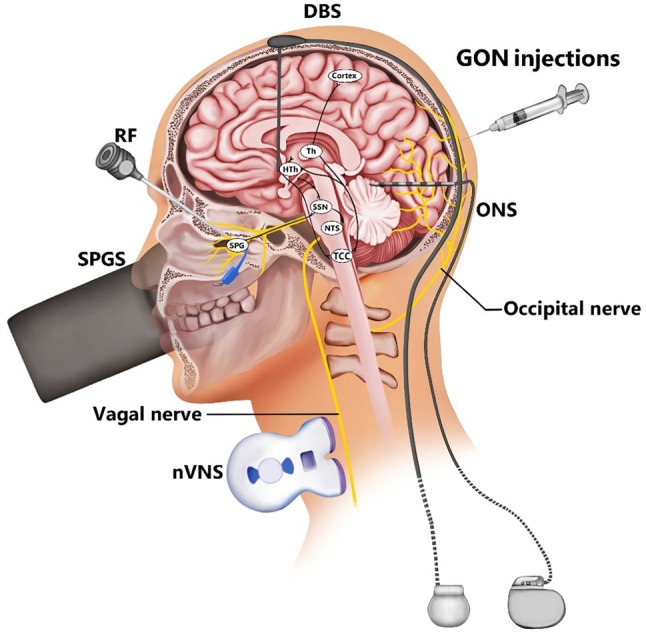
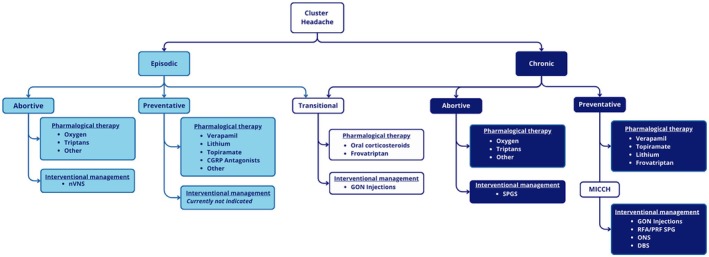
Results: Oxygen therapy and subcutaneous sumatriptan are the most effective abortive treatments for cluster headache. Oral corticosteroid tapering regimens can be used as bridging therapy. Verapamil, lithium, topiramate, and CGRP antagonists are potential preventive medication options. Greater occipital nerve (GON) injections and radiofrequency (RF) therapy can be used as preventive treatments, though their effects are often temporary. For refractory chronic cluster headache, occipital nerve stimulation (ONS) has proven to be effective. Deep brain stimulation (DBS) may also be considered if all other treatments have failed.
Conclusions: The management of cluster headache is complex due to the variable efficacy of treatments across different patients and limited evidence.
期刊介绍:
Pain Practice, the official journal of the World Institute of Pain, publishes international multidisciplinary articles on pain and analgesia that provide its readership with up-to-date research, evaluation methods, and techniques for pain management. Special sections including the Consultant’s Corner, Images in Pain Practice, Case Studies from Mayo, Tutorials, and the Evidence-Based Medicine combine to give pain researchers, pain clinicians and pain fellows in training a systematic approach to continuing education in pain medicine. Prior to publication, all articles and reviews undergo peer review by at least two experts in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


