Alex L Gornitzky, Zoe E Belardo, Bridget K Ellsworth, Sulagna Sarkar, Joseph L Yellin, Arianna Trionfo, Apurva S Shah
{"title":"Pain After Lower Extremity Fracture Surgery: What Is Normal and How Is It Impacted by Individual-specific and Caregiver-specific Psychosocial Factors?","authors":"Alex L Gornitzky, Zoe E Belardo, Bridget K Ellsworth, Sulagna Sarkar, Joseph L Yellin, Arianna Trionfo, Apurva S Shah","doi":"10.1016/j.jposna.2025.100165","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This pilot study characterized normative pain and analgesic consumption following lower-extremity fracture surgery in children. Additionally, we sought to determine how various caregiver- and patient-specific psychosocial factors affect pain, opioid use, and health-related quality-of-life (HRQOL). We hypothesized that the majority of children following lower extremity fracture surgery would not need prolonged opioids, and that higher preoperative anxiety levels would translate into higher postoperative pain and analgesic needs.</p><p><strong>Methods: </strong>This was a prospective cohort study of children aged 5-17 years old undergoing operative fixation of an isolated lower extremity fracture at a single pediatric trauma center. Baseline surveys were administered preoperatively assessing anxiety, pain catastrophizing, and pain self-efficacy. Daily pain scores and analgesic consumption were collected on postoperative days (POD) 1-7, 10, 14, and 21. HRQOL was assessed via PROMIS Global Health, and functional recovery was assessed via PROMIS Mobility. Clinical data were abstracted from the medical record. Descriptive and bivariate statistics were performed.</p><p><strong>Results: </strong>A total of 63 patients with a mean age of 13.0 ± 2.6 years were included. The most common fracture locations were the ankle (49%), tibia (27%), and femur (17%). Mean daily pain scores peaked at 4.5/10 on POD1 and steadily decreased thereafter. By POD3, 62% of patients had mild pain or less (score ≤3/10), and 53% were no longer taking any opioids. The majority of caregivers (55%) and patients (61%) reported pain-related anxiety of ≥6/10 prior to surgery; 76% of caregivers and 50% of patients were at least moderately confident in their ability to adequately manage pain. Neither caregiver nor patient pain-related anxiety or self-efficacy was significantly related to postoperative pain scores, satisfaction with pain management, or opioid consumption. Caregiver pain catastrophizing and generalized anxiety also did not affect patient outcomes. One week after surgery, anxious children had lower average pain scores (1.2 vs 2.7; <i>P</i> = .005) and were less likely to still be using nonopioid analgesics (47% vs 88%, <i>P</i> = .013).</p><p><strong>Conclusions: </strong>This pilot study contributes preliminary data for postoperative pain, analgesic consumption, and functional recovery following operative treatment of lower extremity fractures that can be used to guide prescribing practices and preoperative expectation management/family education. More work is needed to validate and build upon these findings before they can be safely extrapolated to other clinical scenarios and age groups.</p><p><strong>Key concepts: </strong>(1)In this cohort of children following lower extremity fracture surgery of all types, mean daily pain scores peaked at 4.5 on postoperative day one and steadily decreased thereafter.(2)By POD3, most patients had mild pain or less and the majority were no longer taking any opioid analgesics.(3)The majority of children continue to take nonopioid analgesics (acetaminophen and/or ibuprofen) for a week (or longer) after lower extremity fracture surgery.(4)In this cohort, high-anxiety children tended to report lower pain and take fewer opioids after lower extremity fracture surgery.(5)Although baseline pain-related anxiety was not significantly associated with postoperative outcomes, it remained a significant concern for many families and children, suggesting further work is necessary to determine if, and to what extent, targeted interventions might be helpful.</p><p><strong>Level of evidence: </strong>II, prospective cohort study.</p>","PeriodicalId":520850,"journal":{"name":"Journal of the Pediatric Orthopaedic Society of North America","volume":"11 ","pages":"100165"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12088169/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Pediatric Orthopaedic Society of North America","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.jposna.2025.100165","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This pilot study characterized normative pain and analgesic consumption following lower-extremity fracture surgery in children. Additionally, we sought to determine how various caregiver- and patient-specific psychosocial factors affect pain, opioid use, and health-related quality-of-life (HRQOL). We hypothesized that the majority of children following lower extremity fracture surgery would not need prolonged opioids, and that higher preoperative anxiety levels would translate into higher postoperative pain and analgesic needs.
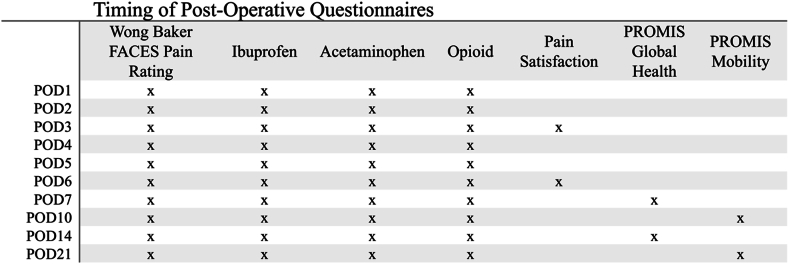
Methods: This was a prospective cohort study of children aged 5-17 years old undergoing operative fixation of an isolated lower extremity fracture at a single pediatric trauma center. Baseline surveys were administered preoperatively assessing anxiety, pain catastrophizing, and pain self-efficacy. Daily pain scores and analgesic consumption were collected on postoperative days (POD) 1-7, 10, 14, and 21. HRQOL was assessed via PROMIS Global Health, and functional recovery was assessed via PROMIS Mobility. Clinical data were abstracted from the medical record. Descriptive and bivariate statistics were performed.
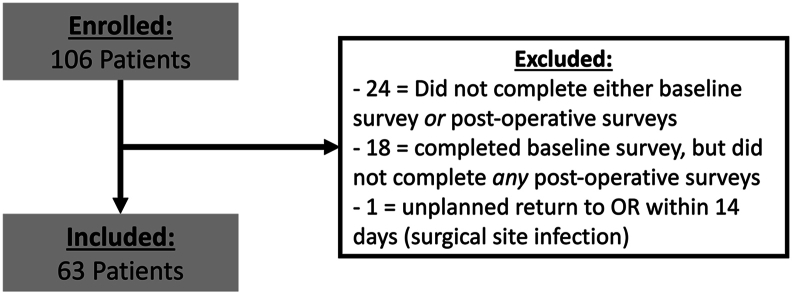
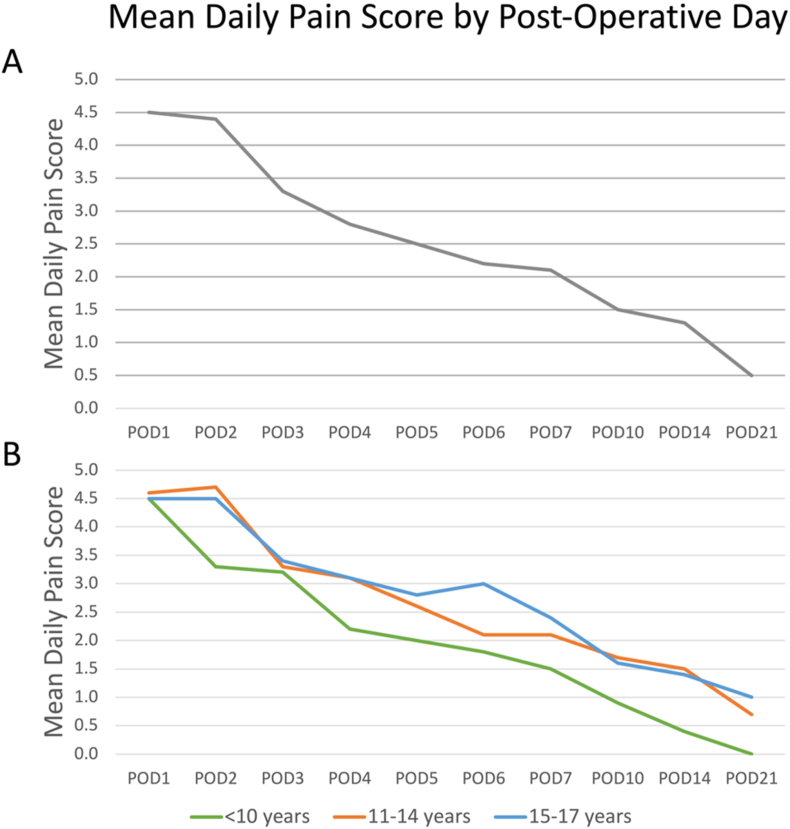
Results: A total of 63 patients with a mean age of 13.0 ± 2.6 years were included. The most common fracture locations were the ankle (49%), tibia (27%), and femur (17%). Mean daily pain scores peaked at 4.5/10 on POD1 and steadily decreased thereafter. By POD3, 62% of patients had mild pain or less (score ≤3/10), and 53% were no longer taking any opioids. The majority of caregivers (55%) and patients (61%) reported pain-related anxiety of ≥6/10 prior to surgery; 76% of caregivers and 50% of patients were at least moderately confident in their ability to adequately manage pain. Neither caregiver nor patient pain-related anxiety or self-efficacy was significantly related to postoperative pain scores, satisfaction with pain management, or opioid consumption. Caregiver pain catastrophizing and generalized anxiety also did not affect patient outcomes. One week after surgery, anxious children had lower average pain scores (1.2 vs 2.7; P = .005) and were less likely to still be using nonopioid analgesics (47% vs 88%, P = .013).
Conclusions: This pilot study contributes preliminary data for postoperative pain, analgesic consumption, and functional recovery following operative treatment of lower extremity fractures that can be used to guide prescribing practices and preoperative expectation management/family education. More work is needed to validate and build upon these findings before they can be safely extrapolated to other clinical scenarios and age groups.
Key concepts: (1)In this cohort of children following lower extremity fracture surgery of all types, mean daily pain scores peaked at 4.5 on postoperative day one and steadily decreased thereafter.(2)By POD3, most patients had mild pain or less and the majority were no longer taking any opioid analgesics.(3)The majority of children continue to take nonopioid analgesics (acetaminophen and/or ibuprofen) for a week (or longer) after lower extremity fracture surgery.(4)In this cohort, high-anxiety children tended to report lower pain and take fewer opioids after lower extremity fracture surgery.(5)Although baseline pain-related anxiety was not significantly associated with postoperative outcomes, it remained a significant concern for many families and children, suggesting further work is necessary to determine if, and to what extent, targeted interventions might be helpful.
背景:本初步研究描述了儿童下肢骨折手术后的疼痛和镇痛药物的使用情况。此外,我们试图确定各种护理者和患者特定的社会心理因素如何影响疼痛、阿片类药物使用和健康相关生活质量(HRQOL)。我们假设大多数下肢骨折手术后的儿童不需要长时间的阿片类药物,并且术前较高的焦虑水平会转化为术后更高的疼痛和镇痛需求。方法:这是一项前瞻性队列研究,研究对象为5-17岁的儿童,他们在单一儿科创伤中心接受了孤立性下肢骨折的手术固定。术前进行基线调查,评估焦虑、疼痛灾难化和疼痛自我效能。术后1-7、10、14和21天分别收集每日疼痛评分和镇痛消耗。HRQOL通过PROMIS Global Health评估,功能恢复通过PROMIS Mobility评估。临床资料从病历中提取。进行描述性和双变量统计。结果:共纳入63例患者,平均年龄13.0±2.6岁。最常见的骨折部位是踝关节(49%)、胫骨(27%)和股骨(17%)。平均每日疼痛评分在POD1时达到4.5/10,此后逐渐下降。到POD3时,62%的患者疼痛轻微或更轻(评分≤3/10),53%的患者不再服用任何阿片类药物。大多数护理人员(55%)和患者(61%)在手术前报告疼痛相关焦虑≥6/10;76%的护理人员和50%的患者对自己充分控制疼痛的能力至少有中等程度的信心。护理者和患者的疼痛相关焦虑或自我效能感与术后疼痛评分、疼痛管理满意度或阿片类药物消费均无显著相关性。照顾者疼痛灾难化和广泛性焦虑也不影响患者的预后。术后一周,焦虑儿童的平均疼痛评分较低(1.2 vs 2.7;P = 0.005),并且仍然使用非阿片类镇痛药的可能性较小(47% vs 88%, P = 0.013)。结论:本初步研究为下肢骨折手术治疗后的术后疼痛、镇痛消耗和功能恢复提供了初步数据,可用于指导处方实践和术前期望管理/家庭教育。需要更多的工作来验证和建立这些发现,然后才能安全地推断到其他临床情况和年龄组。关键概念:(1)在所有类型的下肢骨折手术后的儿童队列中,平均每日疼痛评分在术后第一天达到4.5,此后逐渐下降。(2)到POD3时,大多数患者疼痛轻微或更轻,并且大多数不再服用任何阿片类镇痛药。(3)大多数儿童在下肢骨折手术后继续服用非阿片类镇痛药(对乙酰氨基酚和/或布洛芬)一周(或更长时间)。(5)尽管基线疼痛相关焦虑与术后结局没有显著相关,但许多家庭和儿童仍然非常关注,这表明有针对性的干预措施是否有帮助,以及在多大程度上有帮助,还需要进一步的研究。证据等级:II,前瞻性队列研究。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


