Outcomes of Primary Cementless Total Hip Arthroplasty for Rapidly Destructive Coxarthrosis from Osteonecrosis of the Femoral Head: A Matched Cohort Study.
Ji Hoon Bahk, Joo-Hyoun Song, Young Wook Lim, Cheolsoon Park, Kee-Haeng Lee
{"title":"Outcomes of Primary Cementless Total Hip Arthroplasty for Rapidly Destructive Coxarthrosis from Osteonecrosis of the Femoral Head: A Matched Cohort Study.","authors":"Ji Hoon Bahk, Joo-Hyoun Song, Young Wook Lim, Cheolsoon Park, Kee-Haeng Lee","doi":"10.5371/hp.2025.37.2.112","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Total hip arthroplasty (THA) is the only definitive treatment for rapidly destructive coxarthrosis (RDC). THA for RDC has significantly higher perioperative blood loss with a greater requirement for transfusion than non-RDC primary THAs. Given the rarity of the disease, this study aimed to investigate perioperative and long-term outcomes of cementless THA for RDC that developed from osteonecrosis of the femoral head (ONFH).</p><p><strong>Materials and methods: </strong>Each of 26 RDC patients was matched to a patient with typical advanced-stage ONFH for comparison, according to age, sex, American Society of Anesthesiologists classification, and the type of implant used. As a primary outcome, perioperative blood loss was calculated as the sum of compensated and uncompensated blood loss.</p><p><strong>Results: </strong>The RDC group had a significantly larger amount of total perioperative blood loss in comparison to the group with typical ONFH (791.5 mL vs. 511.2 mL, <i>P</i>=0.034), which was primarily attributable to compensated blood loss (496.1 mL vs. 141.5 mL, <i>P</i>=0.024), as uncompensated blood loss was not significantly different (<i>P</i>=0.152). Intraoperative transfusion volume was significantly higher in the RDC group (234.6 mL vs. 46.2 mL, <i>P</i>=0.007), while the difference in postoperative transfusion was marginally significant (<i>P</i>=0.092).</p><p><strong>Conclusion: </strong>THA for RDC was accompanied by a higher perioperative blood loss, attributable mainly to a significant difference in the amount of intraoperative transfusion, in a matched comparison with patients with typical advanced-stage ONFH. However, extended operation time and prolonged hospitalization along with a large volume of transfusion did not translate into inferior long-term outcomes.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"37 2","pages":"112-119"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2025.37.2.112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Total hip arthroplasty (THA) is the only definitive treatment for rapidly destructive coxarthrosis (RDC). THA for RDC has significantly higher perioperative blood loss with a greater requirement for transfusion than non-RDC primary THAs. Given the rarity of the disease, this study aimed to investigate perioperative and long-term outcomes of cementless THA for RDC that developed from osteonecrosis of the femoral head (ONFH).
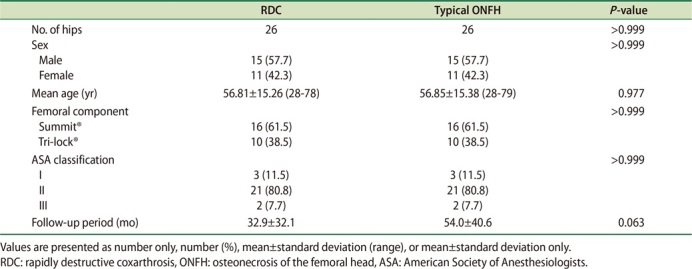
Materials and methods: Each of 26 RDC patients was matched to a patient with typical advanced-stage ONFH for comparison, according to age, sex, American Society of Anesthesiologists classification, and the type of implant used. As a primary outcome, perioperative blood loss was calculated as the sum of compensated and uncompensated blood loss.
Results: The RDC group had a significantly larger amount of total perioperative blood loss in comparison to the group with typical ONFH (791.5 mL vs. 511.2 mL, P=0.034), which was primarily attributable to compensated blood loss (496.1 mL vs. 141.5 mL, P=0.024), as uncompensated blood loss was not significantly different (P=0.152). Intraoperative transfusion volume was significantly higher in the RDC group (234.6 mL vs. 46.2 mL, P=0.007), while the difference in postoperative transfusion was marginally significant (P=0.092).
Conclusion: THA for RDC was accompanied by a higher perioperative blood loss, attributable mainly to a significant difference in the amount of intraoperative transfusion, in a matched comparison with patients with typical advanced-stage ONFH. However, extended operation time and prolonged hospitalization along with a large volume of transfusion did not translate into inferior long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


