Emmanuel Ndenor Sambo, Muhammad Jami Husain, Soumava Basu, Malau Mangai Toma, Sunday Victor Eze, Kufor Osi, Nanlop Ogbureke, Okeoma Erojikwe, Bolanle Banigbe, Andrew E Moran, Deliana Kostova
{"title":"Analysis of costs in implementing the HEARTS hypertension program in Nigerian primary care.","authors":"Emmanuel Ndenor Sambo, Muhammad Jami Husain, Soumava Basu, Malau Mangai Toma, Sunday Victor Eze, Kufor Osi, Nanlop Ogbureke, Okeoma Erojikwe, Bolanle Banigbe, Andrew E Moran, Deliana Kostova","doi":"10.1186/s12962-025-00626-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Nigeria Hypertension Control Initiative (NHCI) program, launched in 2020, integrates hypertension care into primary healthcare using the HEARTS technical package, which includes screening, health counselling, and standardized hypertension treatment protocols. This package has been piloted through NHCI in Kano and Ogun States and in the Federal Capital Territory (FCT) Abuja, as part of the Hypertension Treatment in Nigeria (HTN) project.</p><p><strong>Objective: </strong>To assess the costs of scaling up the HEARTS hypertension control package and compare these costs with those of usual care.</p><p><strong>Methods: </strong>Data on the costs of implementing the HEARTS program were collected from 15 purposively sampled primary health facilities in Kano, Ogun, and FCT Abuja between February and April 2024. Costs included training, medicines, provider time, and administrative expenses. We used the HEARTS costing tool, an Excel-based instrument, to collect and analyze the annual costs from a health system perspective, using an activity-based approach.</p><p><strong>Results: </strong>The estimated annual cost of implementing HEARTS was USD 16 per adult primary care user (PCU), with variations across the three locations: USD 21 in Abuja, USD 11 in Kano, and USD 16 in Ogun. Average annual medication costs per patient treated under HEARTS also varied by location, amounting to USD 28 in Abuja, USD 27 in Ogun, and USD 16 in Kano. Under usual care, annual medication costs per patient were estimated at USD 32 in Kano and USD 16 in Ogun (data for Abuja were unavailable). Major cost drivers for the HEARTS package included provider time (49%) and medication (47%), compared to usual care, where medication alone accounted for 80% of costs. Implementing HEARTS requires a full-time equivalent of 0.45 doctors, 1.59 nurses, and 5.21 community health workers per 10,000 primary care users.</p><p><strong>Conclusions: </strong>In the Nigerian primary care setting, provider time costs and medication costs emerge as major considerations in scaling up hypertension services. Policy options could consider reducing follow-up visit frequency for well-controlled patients to decrease provider time costs. Additionally, medication costs may be reduced by prioritizing first-line treatments and volume-driven purchasing as program scale-up continues.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"23 1","pages":"23"},"PeriodicalIF":2.5000,"publicationDate":"2025-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12117767/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-025-00626-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
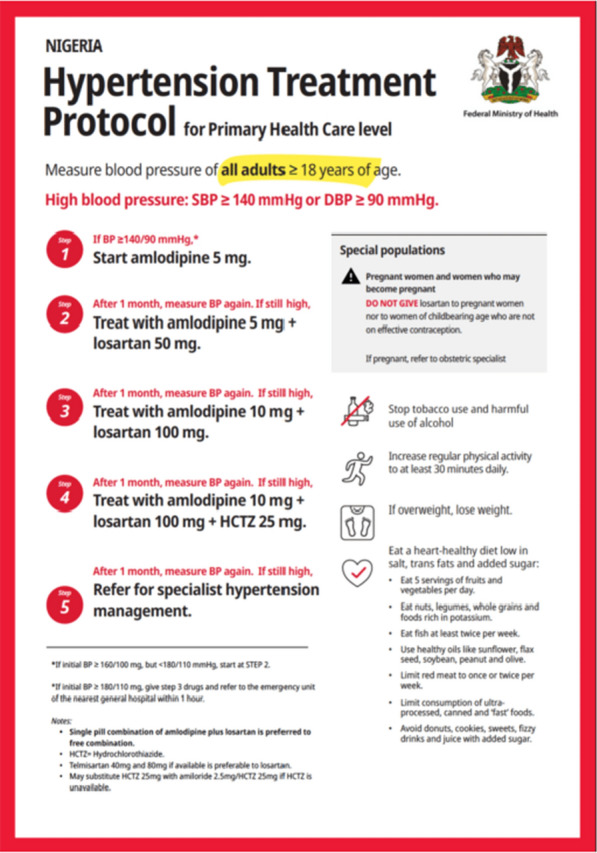
Background: The Nigeria Hypertension Control Initiative (NHCI) program, launched in 2020, integrates hypertension care into primary healthcare using the HEARTS technical package, which includes screening, health counselling, and standardized hypertension treatment protocols. This package has been piloted through NHCI in Kano and Ogun States and in the Federal Capital Territory (FCT) Abuja, as part of the Hypertension Treatment in Nigeria (HTN) project.
Objective: To assess the costs of scaling up the HEARTS hypertension control package and compare these costs with those of usual care.
Methods: Data on the costs of implementing the HEARTS program were collected from 15 purposively sampled primary health facilities in Kano, Ogun, and FCT Abuja between February and April 2024. Costs included training, medicines, provider time, and administrative expenses. We used the HEARTS costing tool, an Excel-based instrument, to collect and analyze the annual costs from a health system perspective, using an activity-based approach.
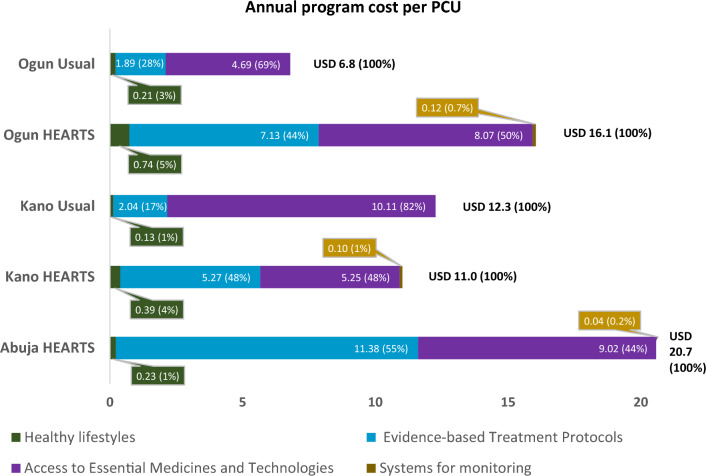
Results: The estimated annual cost of implementing HEARTS was USD 16 per adult primary care user (PCU), with variations across the three locations: USD 21 in Abuja, USD 11 in Kano, and USD 16 in Ogun. Average annual medication costs per patient treated under HEARTS also varied by location, amounting to USD 28 in Abuja, USD 27 in Ogun, and USD 16 in Kano. Under usual care, annual medication costs per patient were estimated at USD 32 in Kano and USD 16 in Ogun (data for Abuja were unavailable). Major cost drivers for the HEARTS package included provider time (49%) and medication (47%), compared to usual care, where medication alone accounted for 80% of costs. Implementing HEARTS requires a full-time equivalent of 0.45 doctors, 1.59 nurses, and 5.21 community health workers per 10,000 primary care users.
Conclusions: In the Nigerian primary care setting, provider time costs and medication costs emerge as major considerations in scaling up hypertension services. Policy options could consider reducing follow-up visit frequency for well-controlled patients to decrease provider time costs. Additionally, medication costs may be reduced by prioritizing first-line treatments and volume-driven purchasing as program scale-up continues.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


