Azadeh Fischer, Nadja Jauert, Martin Schikora, Michael Joebges, Wolfram Doehner
{"title":"The Impact of Concurrent Chronic Heart Failure and Chronic Kidney Dysfunction on Post-Stroke Rehabilitation Outcomes.","authors":"Azadeh Fischer, Nadja Jauert, Martin Schikora, Michael Joebges, Wolfram Doehner","doi":"10.3390/neurolint17050070","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives:</b> The aim of this study was to evaluate the impact of chronic heart failure (CHF), chronic kidney dysfunction (CKD), and the combined CHF-CKD comorbidity on the outcomes of rehabilitation in stroke patients. <b>Methods:</b> A total of 586 patients who had suffered a stroke (mean age, 70 ± 13; 47.6% female; 72.4% ischemic and 27.6% hemorrhagic strokes) and who were admitted immediately after acute stroke care to a rehabilitation center were included in this cohort study and followed up with until their death or discharge from the rehabilitation center. The clinical characteristics of the patients were obtained from their medical records. The relationship between the background comorbidities (CHF, CKD, and concurrent CHF-CKD) and fatal and non-fatal unfavorable outcomes (emergency readmission to a primary hospital or transfer to a long-term care facility in a vegetative or minimally conscious state) were investigated. <b>Results:</b> Unfavorable outcomes were more common in the groups with background CHF and/or CKD. From the Cox multivariate analysis, both CHF and CKD were independent prognostic factors for the occurrence of unfavorable outcomes, with a hazard ratio (HR) of 2.28 (95% CI = 1.2-4.29; <i>p</i>-value = 0.01) and 2.19 (95% CI = 1.24-3.87; <i>p</i>-value = 0.007), respectively. Moreover, the combined CHF-CKD comorbidity showed a more than 5-fold increased risk of an adverse post-stroke outcome (HR of 5.8; 95% CI = 2.5-13.44; <i>p</i>-value < 0.001). <b>Conclusions:</b> The combined CHF-CKD comorbidity is an important independent complicating factor that, along with other known influencing factors, can affect unfavorable post-stroke outcomes more than CHF or CKD alone, and necessitates critical attention to its diagnosis and management as a separate mixed syndrome.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 5","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12113819/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17050070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
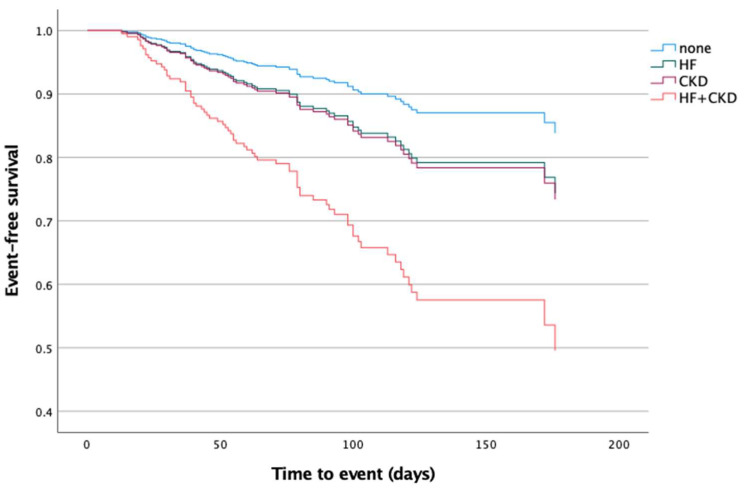
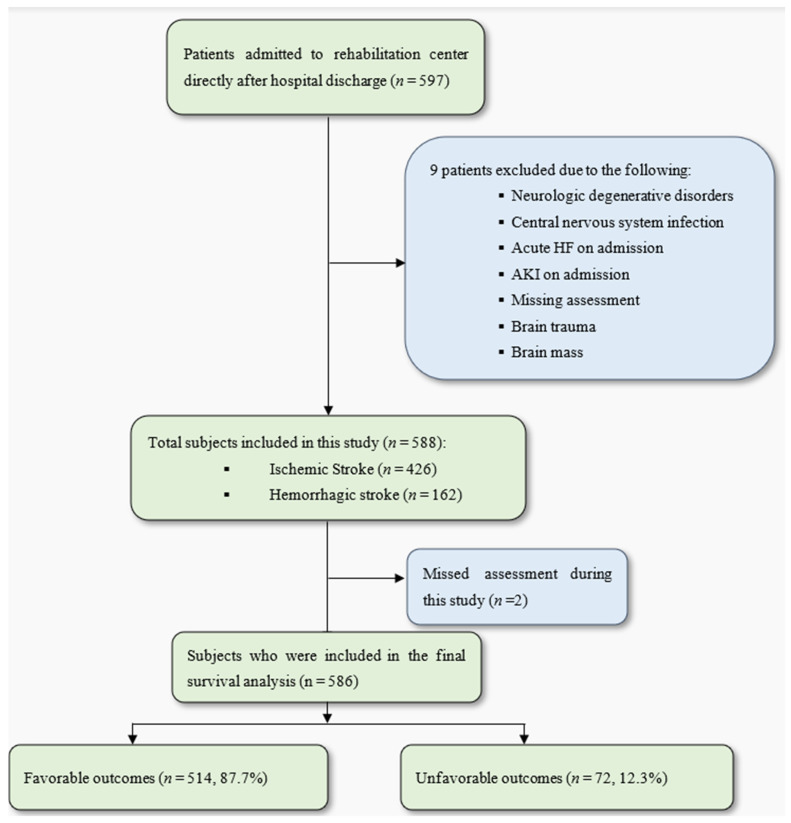
Background/Objectives: The aim of this study was to evaluate the impact of chronic heart failure (CHF), chronic kidney dysfunction (CKD), and the combined CHF-CKD comorbidity on the outcomes of rehabilitation in stroke patients. Methods: A total of 586 patients who had suffered a stroke (mean age, 70 ± 13; 47.6% female; 72.4% ischemic and 27.6% hemorrhagic strokes) and who were admitted immediately after acute stroke care to a rehabilitation center were included in this cohort study and followed up with until their death or discharge from the rehabilitation center. The clinical characteristics of the patients were obtained from their medical records. The relationship between the background comorbidities (CHF, CKD, and concurrent CHF-CKD) and fatal and non-fatal unfavorable outcomes (emergency readmission to a primary hospital or transfer to a long-term care facility in a vegetative or minimally conscious state) were investigated. Results: Unfavorable outcomes were more common in the groups with background CHF and/or CKD. From the Cox multivariate analysis, both CHF and CKD were independent prognostic factors for the occurrence of unfavorable outcomes, with a hazard ratio (HR) of 2.28 (95% CI = 1.2-4.29; p-value = 0.01) and 2.19 (95% CI = 1.24-3.87; p-value = 0.007), respectively. Moreover, the combined CHF-CKD comorbidity showed a more than 5-fold increased risk of an adverse post-stroke outcome (HR of 5.8; 95% CI = 2.5-13.44; p-value < 0.001). Conclusions: The combined CHF-CKD comorbidity is an important independent complicating factor that, along with other known influencing factors, can affect unfavorable post-stroke outcomes more than CHF or CKD alone, and necessitates critical attention to its diagnosis and management as a separate mixed syndrome.
背景/目的:本研究的目的是评估慢性心力衰竭(CHF)、慢性肾功能不全(CKD)以及合并CHF-CKD合并症对脑卒中患者康复结局的影响。方法:586例脑卒中患者(平均年龄70±13岁;47.6%的女性;72.4%的缺血性中风和27.6%的出血性中风)和在急性中风治疗后立即入院的康复中心被纳入本队列研究,并随访至他们死亡或从康复中心出院。从患者的医疗记录中获得患者的临床特征。本研究调查了背景合并症(CHF、CKD和并发CHF-CKD)与致死性和非致死性不良结果(急诊再入院或植物人或最低意识状态下转入长期护理机构)之间的关系。结果:不良结果在背景为CHF和/或CKD的组中更为常见。从Cox多因素分析来看,CHF和CKD都是发生不良结局的独立预后因素,其危险比(HR)为2.28 (95% CI = 1.2-4.29;p值= 0.01)和2.19 (95% CI = 1.24-3.87;p值= 0.007)。此外,合并CHF-CKD合并症显示卒中后不良结果的风险增加了5倍以上(HR为5.8;95% ci = 2.5-13.44;p值< 0.001)。结论:合并CHF-CKD合并症是一个重要的独立并发症因素,与其他已知的影响因素一起,对卒中后不良结局的影响比单独的CHF或CKD更大,需要将其作为单独的混合综合征进行诊断和管理。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


