{"title":"Adjuvant Lenvatinib for High-Risk CNLC IIb/IIIa Hepatocellular Carcinoma After Curative Hepatectomy: A Prospective Exploratory Study.","authors":"Hui-Chuan Sun, Zhi-Yong Huang, Tianfu Wen, Lianxin Liu, Xiao-Dong Zhu, Erlei Zhang, Chuan Li, Xiaoyun Zhang, Jiabei Wang, Jia Fan, Jian Zhou","doi":"10.2147/JHC.S516478","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The risk of hepatocellular carcinoma (HCC) recurrence following surgical resection remains high, approaching 50%-70% at 5 years, with the highest risk occurring in the first year after resection. This study aimed to evaluate the efficacy and safety of lenvatinib as adjuvant therapy for HCC.</p><p><strong>Methods: </strong>In this open-label, single-arm, prospective, multicenter Phase II clinical study, a total of 51 hCC patients with China Liver Cancer (CNLC) stage IIb/IIIa (ie tumor number ≥ 4 or vascular invasion, equivalent to BCLC B/C) who underwent R0 resection 4-6 weeks after curative surgery were enrolled. Patients received lenvatinib for up to 12 months, at a dose of 8 mg/day for body weight < 60 kg, or 12 mg/day for ≥ 60 kg. Patients were followed up every 2 months for a median of 24.1 months.</p><p><strong>Results: </strong>The median recurrence-free survival (RFS) was 16.1 months, with a 12-month RFS rate of 60.4%, exceeding the historical rate of under 50% in similar high-risk populations. The 12-month overall survival (OS) rate was 93.6%, while median OS was not reached. Treatment-related adverse events (TRAEs) occurred in 88.0% of patients, with ≥ grade 3 TRAEs in 14.0%, including thrombocytopenia and proteinuria in 6.0% of patients each, and leukopenia, neutropenia, elevated aspartate aminotransferase, and elevated alanine aminotransferase in 2.0% of patients each. AEs leading to the interruption of lenvatinib occurred in 6.0% of patients, and dose reduction was required in 18% of patients. No deaths were observed.</p><p><strong>Conclusion: </strong>Lenvatinib may be an effective adjuvant therapy for patients with CNLC stage IIb/IIIa HCC after R0 hepatectomy. However, the findings are limited by the single-arm design and small patient cohort, necessitating larger randomized controlled trials for validation.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1043-1056"},"PeriodicalIF":3.4000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12105637/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S516478","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The risk of hepatocellular carcinoma (HCC) recurrence following surgical resection remains high, approaching 50%-70% at 5 years, with the highest risk occurring in the first year after resection. This study aimed to evaluate the efficacy and safety of lenvatinib as adjuvant therapy for HCC.
Methods: In this open-label, single-arm, prospective, multicenter Phase II clinical study, a total of 51 hCC patients with China Liver Cancer (CNLC) stage IIb/IIIa (ie tumor number ≥ 4 or vascular invasion, equivalent to BCLC B/C) who underwent R0 resection 4-6 weeks after curative surgery were enrolled. Patients received lenvatinib for up to 12 months, at a dose of 8 mg/day for body weight < 60 kg, or 12 mg/day for ≥ 60 kg. Patients were followed up every 2 months for a median of 24.1 months.
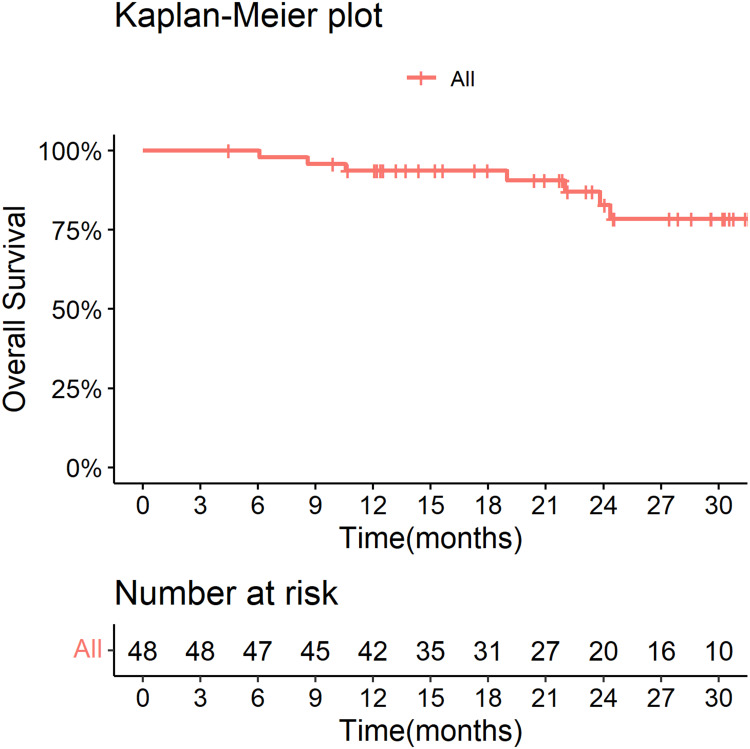
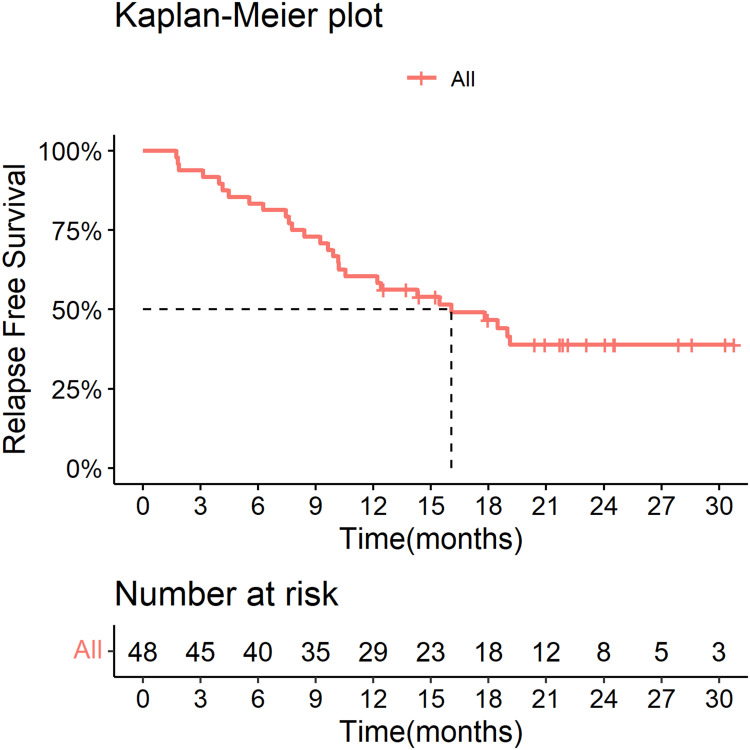
Results: The median recurrence-free survival (RFS) was 16.1 months, with a 12-month RFS rate of 60.4%, exceeding the historical rate of under 50% in similar high-risk populations. The 12-month overall survival (OS) rate was 93.6%, while median OS was not reached. Treatment-related adverse events (TRAEs) occurred in 88.0% of patients, with ≥ grade 3 TRAEs in 14.0%, including thrombocytopenia and proteinuria in 6.0% of patients each, and leukopenia, neutropenia, elevated aspartate aminotransferase, and elevated alanine aminotransferase in 2.0% of patients each. AEs leading to the interruption of lenvatinib occurred in 6.0% of patients, and dose reduction was required in 18% of patients. No deaths were observed.
Conclusion: Lenvatinib may be an effective adjuvant therapy for patients with CNLC stage IIb/IIIa HCC after R0 hepatectomy. However, the findings are limited by the single-arm design and small patient cohort, necessitating larger randomized controlled trials for validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


