Chest tube drainage versus repeated therapeutic thoracentesis for the management of pleural infections: a retrospective multicentre propensity-matched study.
Marion Charron, Victor Roy, Christophe Gut-Gobert, Etienne-Marie Jutant, Louis Leclere, Baptiste Hourmant, Jean-Claude Meurice, Stéphane Jouneau, David Luque Paz
{"title":"Chest tube drainage versus repeated therapeutic thoracentesis for the management of pleural infections: a retrospective multicentre propensity-matched study.","authors":"Marion Charron, Victor Roy, Christophe Gut-Gobert, Etienne-Marie Jutant, Louis Leclere, Baptiste Hourmant, Jean-Claude Meurice, Stéphane Jouneau, David Luque Paz","doi":"10.1186/s41479-025-00167-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Drainage of infected pleural fluid is pivotal in the management of pleural infections, either by chest tube drainage (CTD) or repeated therapeutic thoracocentesis (RTT), in association with the use of intrapleural fibrinolytic therapy (IPFT) and DNase.</p><p><strong>Methods: </strong>The aim of this study was to compare the efficacy and the safety of these two methods of pleural drainage. We conducted a multicenter retrospective study, which included all the patients who was hospitalized for suspected pleural infection in three university hospitals between 2012 and 2021 drained by CTD or RTT. A propensity-score matching was performed to compare patients drained by RTT (RTT group) and by chest tube (CTD group) with adjunctive IPFT and DNase.</p><p><strong>Results: </strong>Two hundred and twenty-nine patients with suspected pleural infection were included. After a propensity-score matching, 78 patients were included in the final analysis, divided in two groups of 39 patients each. Patients in RTT group had a reduced length of drainage (6 days [4.3-8] vs 9 [6.5-13], OR = 1.41, 95%CI [1.05-1.89]) and a reduced length of hospital stay (15 days [11.5-21.5] vs 21 [14-30.5], OR = 1.28, 95%CI [1.01-1.61]). There was no significant difference in mortality rates, surgical referral, relapse, and drainage-related complications between the two groups.</p><p><strong>Conclusions: </strong>The management of pleural infections through RTT with IPFT and DNase appears to be as effective and as safe as CTD. Randomized controlled trials comparing RTT and CTD would be required to confirm these results.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"17 1","pages":"13"},"PeriodicalIF":6.2000,"publicationDate":"2025-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12103787/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-025-00167-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Drainage of infected pleural fluid is pivotal in the management of pleural infections, either by chest tube drainage (CTD) or repeated therapeutic thoracocentesis (RTT), in association with the use of intrapleural fibrinolytic therapy (IPFT) and DNase.
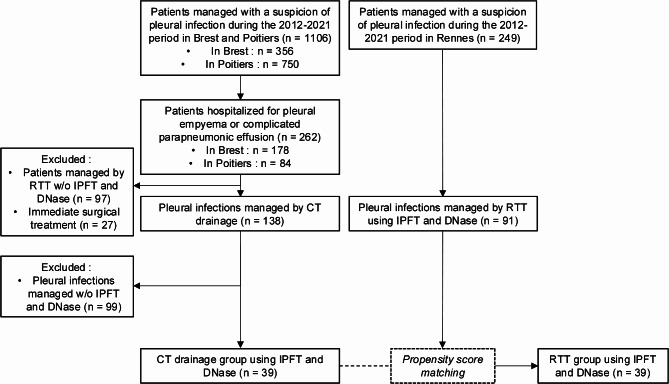
Methods: The aim of this study was to compare the efficacy and the safety of these two methods of pleural drainage. We conducted a multicenter retrospective study, which included all the patients who was hospitalized for suspected pleural infection in three university hospitals between 2012 and 2021 drained by CTD or RTT. A propensity-score matching was performed to compare patients drained by RTT (RTT group) and by chest tube (CTD group) with adjunctive IPFT and DNase.
Results: Two hundred and twenty-nine patients with suspected pleural infection were included. After a propensity-score matching, 78 patients were included in the final analysis, divided in two groups of 39 patients each. Patients in RTT group had a reduced length of drainage (6 days [4.3-8] vs 9 [6.5-13], OR = 1.41, 95%CI [1.05-1.89]) and a reduced length of hospital stay (15 days [11.5-21.5] vs 21 [14-30.5], OR = 1.28, 95%CI [1.01-1.61]). There was no significant difference in mortality rates, surgical referral, relapse, and drainage-related complications between the two groups.
Conclusions: The management of pleural infections through RTT with IPFT and DNase appears to be as effective and as safe as CTD. Randomized controlled trials comparing RTT and CTD would be required to confirm these results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


