Eduard Sidelnikov, Bethany A Kalich, Margot Lisa Miglins, Jasjit K Multani, Rifat Tuly, Kevin Hawkins, Usman Baber
{"title":"Relationship Between Timing of PCSK9 Inhibitor Monoclonal Antibody Initiation and Clinical Outcomes in Patients with Prior Cardiovascular Events.","authors":"Eduard Sidelnikov, Bethany A Kalich, Margot Lisa Miglins, Jasjit K Multani, Rifat Tuly, Kevin Hawkins, Usman Baber","doi":"10.2147/TCRM.S512708","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Timing of initiation of proprotein convertase subtilisin/kexin type 9 inhibitor (PCSK9i) monoclonal antibody (mAb) therapy and its impact on cardiovascular outcomes is unknown. The aim was to identify any association between timing of PCSK9i mAb initiation after a major adverse cardiovascular event (MACE) and the rate of subsequent MACE.</p><p><strong>Patient and methods: </strong>A retrospective cohort study of adult patients in the United States with a MACE (myocardial infarction, stroke, unstable angina, or coronary revascularization) from January 1, 2017 to February 28, 2022 was conducted using administrative claims databases (index date = first observed MACE during this period). Patients were required to have ≥360 days of data visibility prior to (baseline period) and for ≥30 days after the index date (minimum, variable follow up period), and ≥1 prescription claim for PCSK9i mAb therapy on or after the index date. Subsequent MACE rates, time from index MACE to PCSK9i mAb initiation, and time to subsequent MACE were reported.</p><p><strong>Results: </strong>A total of 58,997 patients with ≥1 MACE were identified (mean age = 64 years; 58% male; median follow up=1,241 days). Over half of the patients did not initiate a PCSK9i mAb in the first year after the index MACE. Overall, 35% (n = 20,465) had ≥1 subsequent MACE. Compared to the period between index MACE and prior to PCSK9i mAb initiation, rates of subsequent MACE after PCSK9i mAb initiation were reduced in a time-dependent manner by 70% among patients who initiated PCSK9i mAb therapy within 30 days, 78% (31-90 days), 76% (91-180 days), 65% (181-360 days), and 42% (>360 days) after the index MACE. Those who initiated PCSK9i mAb within 30 days of the index MACE had longer median time to the first subsequent MACE (111 days) compared to patients who initiated at later times.</p><p><strong>Conclusion: </strong>This study provides evidence that earlier initiation of PCSK9i mAb therapy after a MACE appeared to be associated with longer time to a subsequent MACE. Patients without timely treatment are left at an unnecessarily elevated risk of further MACE.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"727-736"},"PeriodicalIF":2.8000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12103851/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S512708","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Timing of initiation of proprotein convertase subtilisin/kexin type 9 inhibitor (PCSK9i) monoclonal antibody (mAb) therapy and its impact on cardiovascular outcomes is unknown. The aim was to identify any association between timing of PCSK9i mAb initiation after a major adverse cardiovascular event (MACE) and the rate of subsequent MACE.
Patient and methods: A retrospective cohort study of adult patients in the United States with a MACE (myocardial infarction, stroke, unstable angina, or coronary revascularization) from January 1, 2017 to February 28, 2022 was conducted using administrative claims databases (index date = first observed MACE during this period). Patients were required to have ≥360 days of data visibility prior to (baseline period) and for ≥30 days after the index date (minimum, variable follow up period), and ≥1 prescription claim for PCSK9i mAb therapy on or after the index date. Subsequent MACE rates, time from index MACE to PCSK9i mAb initiation, and time to subsequent MACE were reported.
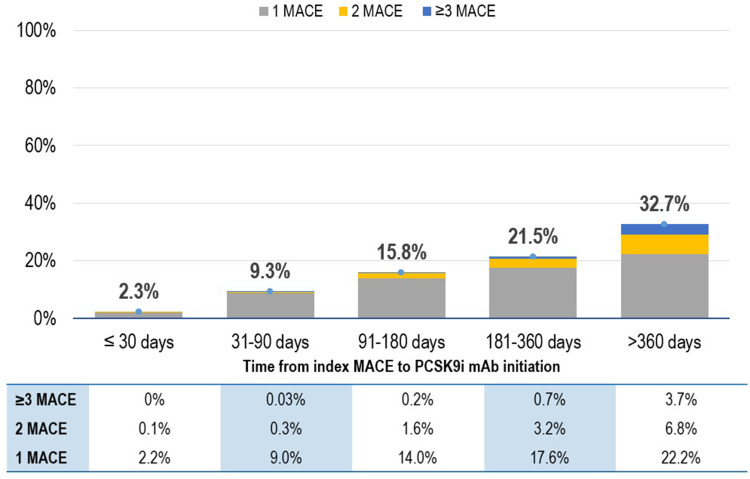
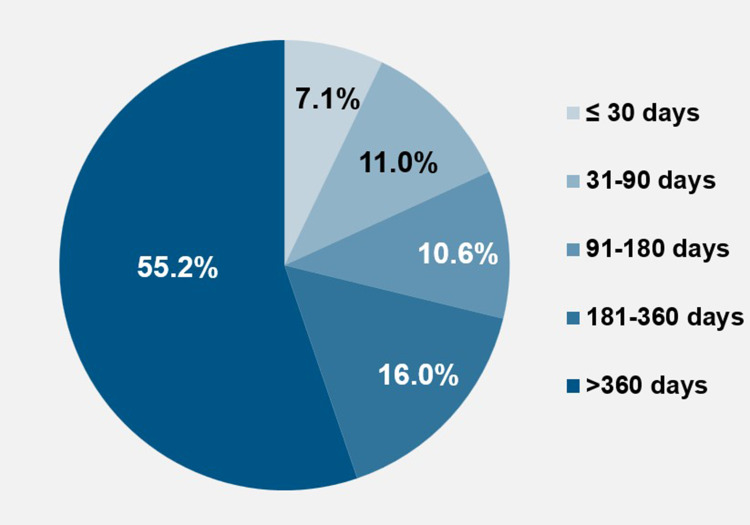
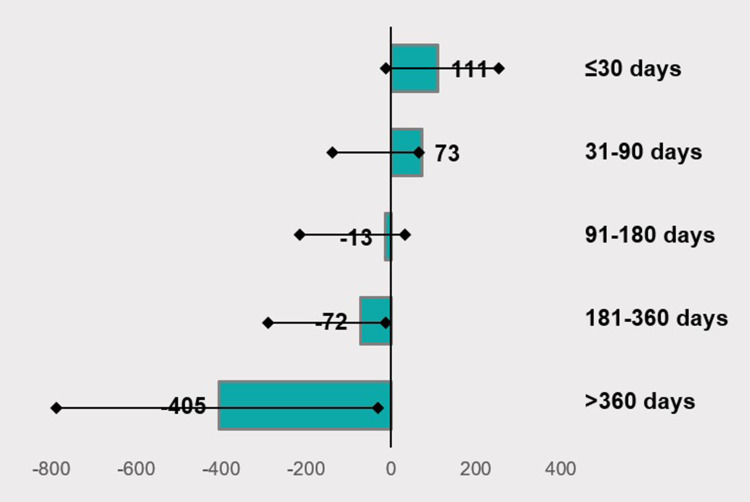
Results: A total of 58,997 patients with ≥1 MACE were identified (mean age = 64 years; 58% male; median follow up=1,241 days). Over half of the patients did not initiate a PCSK9i mAb in the first year after the index MACE. Overall, 35% (n = 20,465) had ≥1 subsequent MACE. Compared to the period between index MACE and prior to PCSK9i mAb initiation, rates of subsequent MACE after PCSK9i mAb initiation were reduced in a time-dependent manner by 70% among patients who initiated PCSK9i mAb therapy within 30 days, 78% (31-90 days), 76% (91-180 days), 65% (181-360 days), and 42% (>360 days) after the index MACE. Those who initiated PCSK9i mAb within 30 days of the index MACE had longer median time to the first subsequent MACE (111 days) compared to patients who initiated at later times.
Conclusion: This study provides evidence that earlier initiation of PCSK9i mAb therapy after a MACE appeared to be associated with longer time to a subsequent MACE. Patients without timely treatment are left at an unnecessarily elevated risk of further MACE.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


