Necessary Intensity of Monitoring After Elective Craniotomies: A Prediction Score for Postoperative Complications to Stratify Postoperative Monitoring.
Elena Kurz, Darius Kalasauskas, Dominik Wesp, Harald Krenzlin, Alicia Schulze, Melek Bulut, Thomas Kerz, Florian Ringel, Naureen Keric
{"title":"Necessary Intensity of Monitoring After Elective Craniotomies: A Prediction Score for Postoperative Complications to Stratify Postoperative Monitoring.","authors":"Elena Kurz, Darius Kalasauskas, Dominik Wesp, Harald Krenzlin, Alicia Schulze, Melek Bulut, Thomas Kerz, Florian Ringel, Naureen Keric","doi":"10.1007/s12028-025-02242-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postoperative complications requiring monitoring following elective craniotomies occur in ~ 2% of cases. Therefore, in most neurosurgical departments, an elective craniotomy is routinely followed by postoperative monitoring in an intensive or intermediate care unit. However, there is no systematic allocation to this procedure. Consequently, patients at risk are not monitored as a priority. The aim of this study was to develop a prediction score for the occurrence of postoperative complications after elective craniotomies and to redefine the monitoring algorithm.</p><p><strong>Methods: </strong>In this retrospective single-center analysis, all patients with elective craniotomy between 2018 and 2021 were included. Demographic data, diagnosis, location of the pathology (infratentorial/supratentorial), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), duration of surgery, blood loss, postoperative complications, and type and duration of monitoring were analyzed. The score was developed and validated internally to ensure its predictive reliability.</p><p><strong>Results: </strong>A total of 860 consecutive patients (376 male patients and 484 female patients) with a mean age of 60.6 years (range 19-93 years) were included. Forty-three patients experienced a postoperative adverse event that required monitoring. Independent predictors for postoperative complications were age (odds ratio [OR] 0.001, 95% confidence interval [CI] 1.0-1.04), CCI (OR 1.19, 95% CI 1.04-1.36), operative duration (OR 45.90, 95% CI 10.01-229.30), vestibular schwannoma as the treated pathology (OR 1.58, 95% CI 0.09-0.77), blood loss (OR 1.001, 95% CI 1.00-1.001), and ASA score (OR 1.1, 95% CI 1.01-1.2). The score was based on the most reliable characteristics and the calculated predictor error. The formula for score calculation is as follows: 1.3 age + 10 CCI + 65 1<sub>{vascular pathology = yes}</sub> + 0.5 duration of surgery + 20.5 ASA score - 100. The discriminatory value for clinical outcomes achieved an area under the curve of 0.78 in validation data.</p><p><strong>Conclusions: </strong>This score provides a practical approach for individual risk assessment of patients undergoing elective craniotomy. Postoperative monitoring capacity can be optimally distributed, and fast-track pathways can be developed for low-risk patients to use this valuable resource effectively.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"484-492"},"PeriodicalIF":3.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436460/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-025-02242-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Postoperative complications requiring monitoring following elective craniotomies occur in ~ 2% of cases. Therefore, in most neurosurgical departments, an elective craniotomy is routinely followed by postoperative monitoring in an intensive or intermediate care unit. However, there is no systematic allocation to this procedure. Consequently, patients at risk are not monitored as a priority. The aim of this study was to develop a prediction score for the occurrence of postoperative complications after elective craniotomies and to redefine the monitoring algorithm.
Methods: In this retrospective single-center analysis, all patients with elective craniotomy between 2018 and 2021 were included. Demographic data, diagnosis, location of the pathology (infratentorial/supratentorial), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), duration of surgery, blood loss, postoperative complications, and type and duration of monitoring were analyzed. The score was developed and validated internally to ensure its predictive reliability.
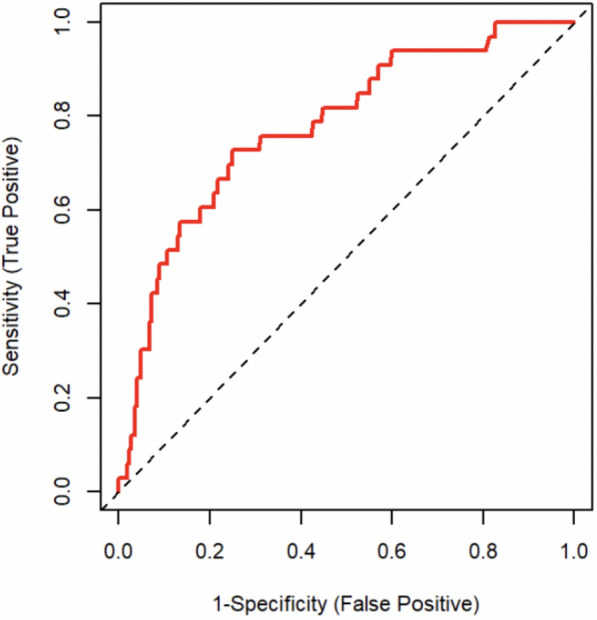
Results: A total of 860 consecutive patients (376 male patients and 484 female patients) with a mean age of 60.6 years (range 19-93 years) were included. Forty-three patients experienced a postoperative adverse event that required monitoring. Independent predictors for postoperative complications were age (odds ratio [OR] 0.001, 95% confidence interval [CI] 1.0-1.04), CCI (OR 1.19, 95% CI 1.04-1.36), operative duration (OR 45.90, 95% CI 10.01-229.30), vestibular schwannoma as the treated pathology (OR 1.58, 95% CI 0.09-0.77), blood loss (OR 1.001, 95% CI 1.00-1.001), and ASA score (OR 1.1, 95% CI 1.01-1.2). The score was based on the most reliable characteristics and the calculated predictor error. The formula for score calculation is as follows: 1.3 age + 10 CCI + 65 1{vascular pathology = yes} + 0.5 duration of surgery + 20.5 ASA score - 100. The discriminatory value for clinical outcomes achieved an area under the curve of 0.78 in validation data.
Conclusions: This score provides a practical approach for individual risk assessment of patients undergoing elective craniotomy. Postoperative monitoring capacity can be optimally distributed, and fast-track pathways can be developed for low-risk patients to use this valuable resource effectively.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


