Valentina Lahn, Sascha R Tittel, Ute Ohlenschläger, Clemens Kamrath, Johanna Hammersen, Renata Gellai, Kirsten Mönkemöller, Axel Dost, Heike Bartelt, Reinhard W Holl
{"title":"Remission Period in Children With Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic-Results From the DPV Registry.","authors":"Valentina Lahn, Sascha R Tittel, Ute Ohlenschläger, Clemens Kamrath, Johanna Hammersen, Renata Gellai, Kirsten Mönkemöller, Axel Dost, Heike Bartelt, Reinhard W Holl","doi":"10.1155/pedi/9903467","DOIUrl":null,"url":null,"abstract":"<p><p>To investigate whether the remission period in type 1 diabetes, as measured by insulin-dose adjusted A1c (IDAA1C), was affected by the COVID-19 pandemic. Data from 7603 children and adolescents with type 1 diabetes from the prospective diabetes follow-up (DPV) registry were available. We compared two time periods of diabetes onset, 2020/2021 vs. 2018/2019. IDAA1C and remission prevalence (IDAA1c < 9%) were analyzed using logistic and linear regression models adjusted for age groups (0.5-<6, 6-<12, and 12-<18 years), sex, diabetic ketoacidosis (DKA) at onset, use of continuous glucose monitoring (CGM) systems, insulin pumps, sensor-augmented pumps (SAPs) or automated insulin delivery (AID) systems, BMI categories (<90. percentile of BMI, 90. -<97. percentile of BMI, 97. -<99.5 percentile of BMI, > = 99.5 percentile of BMI) and immigrant background. Data from three time periods were analyzed: 3-5 months, 6-10 months, and 11-13 months after diagnosis of type 1 diabetes. Compared to the prepandemic period, during the COVID-19 pandemic adjusted IDAA1C was significantly higher at 3-5 months after diagnosis (mean estimated differences 0.26 [95% confidence interval 0.17; 0.35], <i>p</i> < 0.001), but not at 6-10 months and 11-13 months after diagnosis (mean estimated difference 0.08 [-0.01; 0.17], <i>p</i>=0.07; and -0.03 [-0.12; 0.07], <i>p</i>=0.60), reflecting a lower percentage of patients in remission at 3-5 months. Reasons may be changes in autoimmune progression during the pandemic, lack of physical activities, increased stress or psychological burden, or altered access to care with delayed diagnosis of diabetes. Underlying causes need to be evaluated in future studies.</p>","PeriodicalId":19797,"journal":{"name":"Pediatric Diabetes","volume":"2025 ","pages":"9903467"},"PeriodicalIF":5.6000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097864/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Diabetes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/pedi/9903467","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
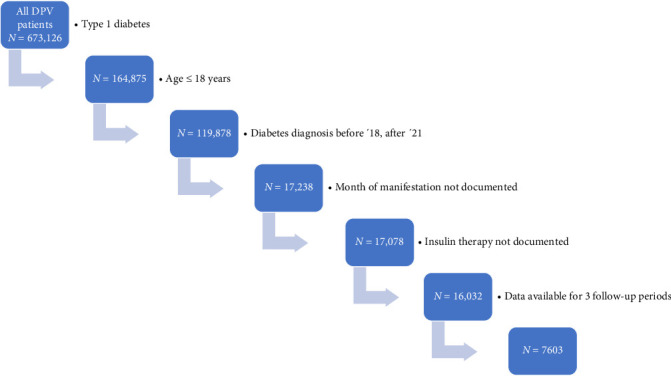
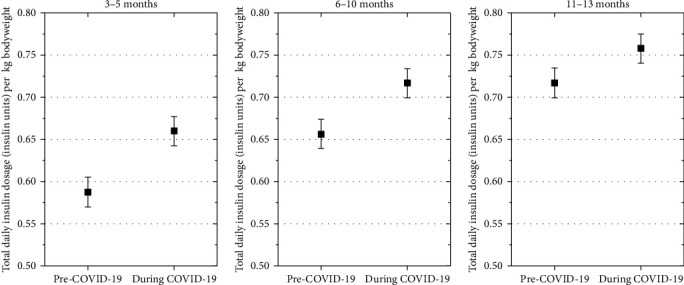
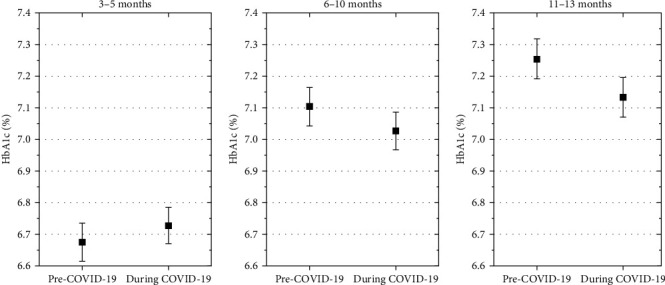
To investigate whether the remission period in type 1 diabetes, as measured by insulin-dose adjusted A1c (IDAA1C), was affected by the COVID-19 pandemic. Data from 7603 children and adolescents with type 1 diabetes from the prospective diabetes follow-up (DPV) registry were available. We compared two time periods of diabetes onset, 2020/2021 vs. 2018/2019. IDAA1C and remission prevalence (IDAA1c < 9%) were analyzed using logistic and linear regression models adjusted for age groups (0.5-<6, 6-<12, and 12-<18 years), sex, diabetic ketoacidosis (DKA) at onset, use of continuous glucose monitoring (CGM) systems, insulin pumps, sensor-augmented pumps (SAPs) or automated insulin delivery (AID) systems, BMI categories (<90. percentile of BMI, 90. -<97. percentile of BMI, 97. -<99.5 percentile of BMI, > = 99.5 percentile of BMI) and immigrant background. Data from three time periods were analyzed: 3-5 months, 6-10 months, and 11-13 months after diagnosis of type 1 diabetes. Compared to the prepandemic period, during the COVID-19 pandemic adjusted IDAA1C was significantly higher at 3-5 months after diagnosis (mean estimated differences 0.26 [95% confidence interval 0.17; 0.35], p < 0.001), but not at 6-10 months and 11-13 months after diagnosis (mean estimated difference 0.08 [-0.01; 0.17], p=0.07; and -0.03 [-0.12; 0.07], p=0.60), reflecting a lower percentage of patients in remission at 3-5 months. Reasons may be changes in autoimmune progression during the pandemic, lack of physical activities, increased stress or psychological burden, or altered access to care with delayed diagnosis of diabetes. Underlying causes need to be evaluated in future studies.
期刊介绍:
Pediatric Diabetes is a bi-monthly journal devoted to disseminating new knowledge relating to the epidemiology, etiology, pathogenesis, management, complications and prevention of diabetes in childhood and adolescence. The aim of the journal is to become the leading vehicle for international dissemination of research and practice relating to diabetes in youth. Papers are considered for publication based on the rigor of scientific approach, novelty, and importance for understanding mechanisms involved in the epidemiology and etiology of this disease, especially its molecular, biochemical and physiological aspects. Work relating to the clinical presentation, course, management and outcome of diabetes, including its physical and emotional sequelae, is considered. In vitro studies using animal or human tissues, whole animal and clinical studies in humans are also considered. The journal reviews full-length papers, preliminary communications with important new information, clinical reports, and reviews of major topics. Invited editorials, commentaries, and perspectives are a regular feature. The editors, based in the USA, Europe, and Australasia, maintain regular communications to assure rapid turnaround time of submitted manuscripts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


