The development and validation of biomarkers-based scoring systems for predicting early recurrence in patients with borderline resectable pancreatic cancer undergoing resection after neoadjuvant therapy.
Hang He, Cai-Feng Zou, Yong-Jian Jiang, Feng Yang, Yang Di, Ji Li, Chen Jin, De-Liang Fu
{"title":"The development and validation of biomarkers-based scoring systems for predicting early recurrence in patients with borderline resectable pancreatic cancer undergoing resection after neoadjuvant therapy.","authors":"Hang He, Cai-Feng Zou, Yong-Jian Jiang, Feng Yang, Yang Di, Ji Li, Chen Jin, De-Liang Fu","doi":"10.21037/gs-2024-500","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant therapy (NAT) is a key component of the treatment strategy for borderline resectable pancreatic cancer (BRPC). However, early recurrence (ER) frequently occurs, leading to a poor prognosis. Effective approaches for ER risk stratification in patients with BRPC undergoing NAT have not been well established currently. This study aimed to develop biomarker-based perioperative scoring systems to predict ER in patients with BRPC who underwent resection after NAT.</p><p><strong>Methods: </strong>Patients with BRPC who underwent radical resection following NAT at our institute between 2018 and 2023 were retrospectively enrolled. Serum biochemical marker tests and imaging examinations were performed to evaluate recurrence. Perioperative biochemical and clinicopathological parameters were analyzed. Univariate and multivariate Cox regression analyses were performed to identify independent risk factors for recurrence and to construct nomograms for ER prediction. Internal validation was conducted using the bootstrapping method. The accuracy in predicting ER was evaluated using receiver operating characteristic curve analysis. Survival analysis was performed using the Kaplan-Meier survival plots and log-rank test.</p><p><strong>Results: </strong>A total of 194 patients were enrolled. Recurrence occurred in 69.0% of all patients, and 61.1% of all recurrences were found within 6 months postoperatively. A preoperative scoring system was developed based on preoperative carbohydrate antigen 19-9 (CA19-9) and CA125 levels to predict ER [area under the curve (AUC), 0.700; 95% confidence interval (95% CI): 0.614-0.786] with 86.4% specificity and 48.7% sensitivity (cut-off value was 0.35886). Patients with a post-NAT prognostic score (PNPS) ≥0.35886 exhibited significantly poorer recurrence-free survival (RFS) (P<0.001) and overall survival (OS) (P<0.001) than those with a PNPS <0.35886. A postoperative scoring system based on the postoperative CA19-9 response was established to predict ER (AUC, 0.785; 95% CI: 0.705-0.866) with 65.4% specificity and 80.8% sensitivity (cut-off value was 0.43949). Patients with a postoperative prognostic score (PPS) ≥0.43949 exhibited poorer RFS (P<0.001) and OS (P<0.001) than those with a PPS <0.43949. For patients with normal CA19-9 levels after NAT, PNPS ≥0.35886 or PPS ≥0.43949 indicated a poor prognosis after surgery. For patients without normal CA19-9 levels after NAT, PNPS <0.35886 or PPS <0.43949 was associated with a favorable prognosis after surgery.</p><p><strong>Conclusions: </strong>The preoperative and postoperative scoring systems provide risk stratification for ER in patients with BRPC undergoing NAT. This may provide references to clinicians in identifying suitable candidates and optimal timing for surgery during NAT, and administering tailored adjuvant therapy (AT) after surgery.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 4","pages":"670-686"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093163/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2024-500","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neoadjuvant therapy (NAT) is a key component of the treatment strategy for borderline resectable pancreatic cancer (BRPC). However, early recurrence (ER) frequently occurs, leading to a poor prognosis. Effective approaches for ER risk stratification in patients with BRPC undergoing NAT have not been well established currently. This study aimed to develop biomarker-based perioperative scoring systems to predict ER in patients with BRPC who underwent resection after NAT.
Methods: Patients with BRPC who underwent radical resection following NAT at our institute between 2018 and 2023 were retrospectively enrolled. Serum biochemical marker tests and imaging examinations were performed to evaluate recurrence. Perioperative biochemical and clinicopathological parameters were analyzed. Univariate and multivariate Cox regression analyses were performed to identify independent risk factors for recurrence and to construct nomograms for ER prediction. Internal validation was conducted using the bootstrapping method. The accuracy in predicting ER was evaluated using receiver operating characteristic curve analysis. Survival analysis was performed using the Kaplan-Meier survival plots and log-rank test.
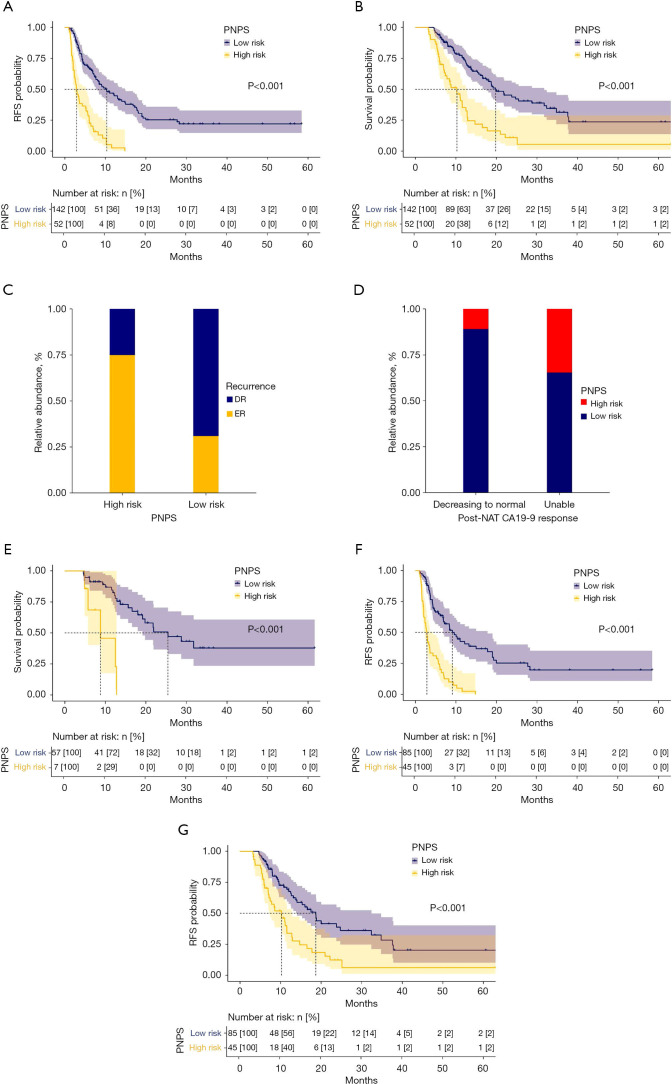
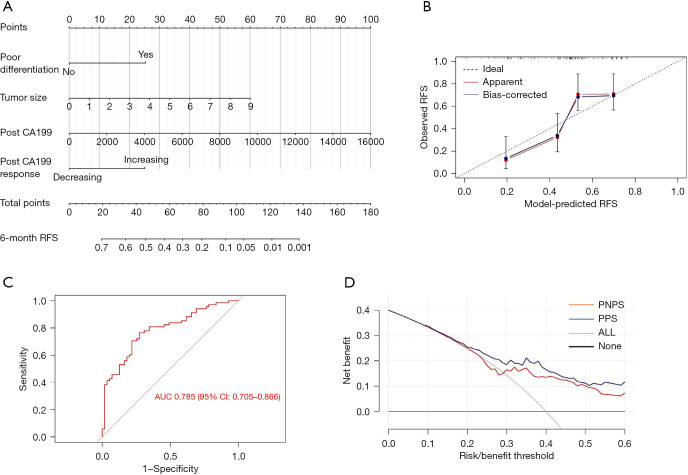
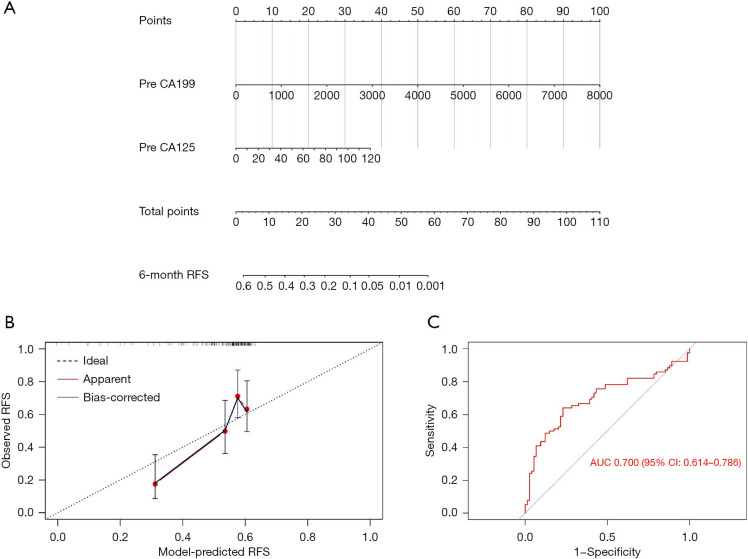
Results: A total of 194 patients were enrolled. Recurrence occurred in 69.0% of all patients, and 61.1% of all recurrences were found within 6 months postoperatively. A preoperative scoring system was developed based on preoperative carbohydrate antigen 19-9 (CA19-9) and CA125 levels to predict ER [area under the curve (AUC), 0.700; 95% confidence interval (95% CI): 0.614-0.786] with 86.4% specificity and 48.7% sensitivity (cut-off value was 0.35886). Patients with a post-NAT prognostic score (PNPS) ≥0.35886 exhibited significantly poorer recurrence-free survival (RFS) (P<0.001) and overall survival (OS) (P<0.001) than those with a PNPS <0.35886. A postoperative scoring system based on the postoperative CA19-9 response was established to predict ER (AUC, 0.785; 95% CI: 0.705-0.866) with 65.4% specificity and 80.8% sensitivity (cut-off value was 0.43949). Patients with a postoperative prognostic score (PPS) ≥0.43949 exhibited poorer RFS (P<0.001) and OS (P<0.001) than those with a PPS <0.43949. For patients with normal CA19-9 levels after NAT, PNPS ≥0.35886 or PPS ≥0.43949 indicated a poor prognosis after surgery. For patients without normal CA19-9 levels after NAT, PNPS <0.35886 or PPS <0.43949 was associated with a favorable prognosis after surgery.
Conclusions: The preoperative and postoperative scoring systems provide risk stratification for ER in patients with BRPC undergoing NAT. This may provide references to clinicians in identifying suitable candidates and optimal timing for surgery during NAT, and administering tailored adjuvant therapy (AT) after surgery.
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


