Recent changes in surgical outcomes and preoperative biliary drainage with the increased use of neoadjuvant chemotherapy in pancreatic cancer patients undergoing pancreatoduodenectomy: a single-center retrospective study.
{"title":"Recent changes in surgical outcomes and preoperative biliary drainage with the increased use of neoadjuvant chemotherapy in pancreatic cancer patients undergoing pancreatoduodenectomy: a single-center retrospective study.","authors":"Naoya Imamura, Atsushi Nanashima, Yuki Tsuchimochi, Takeomi Hamada, Hiroshi Kawakami, Masahide Hiyoshi","doi":"10.21037/gs-2024-507","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant chemotherapy (NAC) has been increasingly used in recent years in patients with pancreatic ductal adenocarcinoma (PDAC). This has forced a change in the practice of preoperative biliary drainage (PBD) is performed in PDAC patients scheduled for pancreatoduodenectomy (PD). What has changed in the NAC era and what is the appropriate method of PBD? To address this question, this study retrospectively reviewed the surgical outcomes and details of PBD in NAC and upfront surgery (US) patients.</p><p><strong>Methods: </strong>The study included consecutive PDAC patients who underwent PD from 2013 to 2021 during the transition from US to NAC, when outcomes were comparable. Clinical factors such as patient background, preoperative examination, surgical procedure, and postoperative complications were compared between the NAC group (40 patients) and the US group (59 patients), and details of PBD such as PBD procedure and adverse events were compared between the NAC and US groups who received PBD (27 NAC patients, 33 US patients). In the comparison test between groups, Fisher's exact test and Mann-Whitney <i>U</i> test were mainly used. In addition, the outcomes and patency periods of each of the 128 PBD procedures were examined for the 60 patients who underwent PBD. The log-rank test was performed using the Kaplan-Meier method to compare patency period by PBD procedure.</p><p><strong>Results: </strong>There were no differences in patient background between the NAC and US groups. Compared with the US group, the NAC group had higher preoperative albumin (ALB) levels and less blood loss, but there was no difference of postoperative complications (NAC <i>vs.</i> US, 35% <i>vs.</i> 46%, respectively, P=0.29). With respect to PBD, the NAC group had more initial metallic stent (MS) placement (NAC <i>vs.</i> US, 52% <i>vs.</i> 15%, respectively, P=0.009), and fewer PBD-related adverse events (NAC <i>vs.</i> US, 33% <i>vs.</i> 61%, respectively, P=0.04). In a comparison of outcomes by drainage method, the duration of patency was significantly longer with MS placement than plastic stent (PS) placement (median days of patency, MS <i>vs.</i> PS, 68 <i>vs.</i> 15 days, respectively, P<0.001). However, MS placement and PS placement were equally likely to require a delay in the surgical schedule due to PBD-related adverse events (MS <i>vs.</i> PS, 6% <i>vs.</i> 6%, respectively, P>0.99).</p><p><strong>Conclusions: </strong>Prolonged PBD with NAC did not adversely affect surgical outcomes. MS placement provides a long patency period and is currently useful in PBD for PDAC patients undergoing PD after NAC, which requires a prolonged preoperative period. However, MS placement also has adverse events, and further studies are needed.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 4","pages":"714-725"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093172/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2024-507","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neoadjuvant chemotherapy (NAC) has been increasingly used in recent years in patients with pancreatic ductal adenocarcinoma (PDAC). This has forced a change in the practice of preoperative biliary drainage (PBD) is performed in PDAC patients scheduled for pancreatoduodenectomy (PD). What has changed in the NAC era and what is the appropriate method of PBD? To address this question, this study retrospectively reviewed the surgical outcomes and details of PBD in NAC and upfront surgery (US) patients.
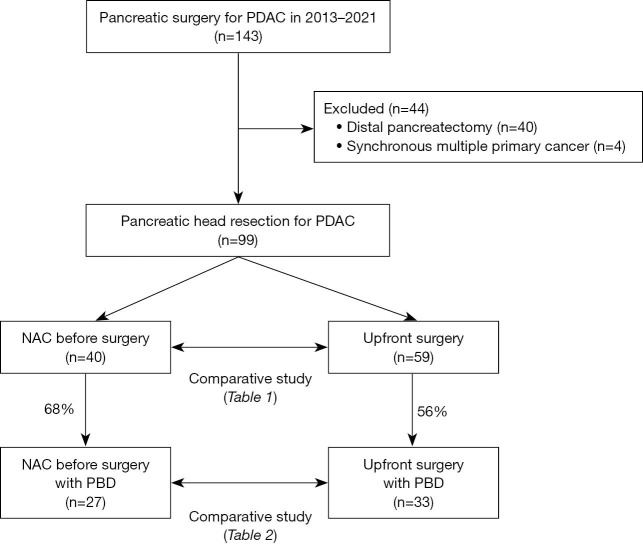
Methods: The study included consecutive PDAC patients who underwent PD from 2013 to 2021 during the transition from US to NAC, when outcomes were comparable. Clinical factors such as patient background, preoperative examination, surgical procedure, and postoperative complications were compared between the NAC group (40 patients) and the US group (59 patients), and details of PBD such as PBD procedure and adverse events were compared between the NAC and US groups who received PBD (27 NAC patients, 33 US patients). In the comparison test between groups, Fisher's exact test and Mann-Whitney U test were mainly used. In addition, the outcomes and patency periods of each of the 128 PBD procedures were examined for the 60 patients who underwent PBD. The log-rank test was performed using the Kaplan-Meier method to compare patency period by PBD procedure.
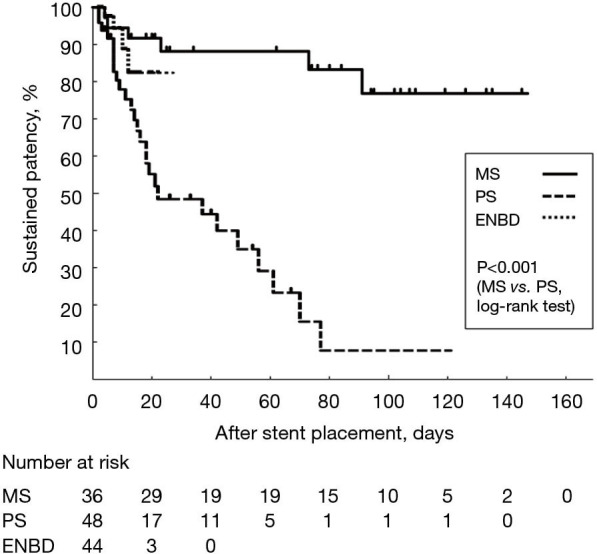
Results: There were no differences in patient background between the NAC and US groups. Compared with the US group, the NAC group had higher preoperative albumin (ALB) levels and less blood loss, but there was no difference of postoperative complications (NAC vs. US, 35% vs. 46%, respectively, P=0.29). With respect to PBD, the NAC group had more initial metallic stent (MS) placement (NAC vs. US, 52% vs. 15%, respectively, P=0.009), and fewer PBD-related adverse events (NAC vs. US, 33% vs. 61%, respectively, P=0.04). In a comparison of outcomes by drainage method, the duration of patency was significantly longer with MS placement than plastic stent (PS) placement (median days of patency, MS vs. PS, 68 vs. 15 days, respectively, P<0.001). However, MS placement and PS placement were equally likely to require a delay in the surgical schedule due to PBD-related adverse events (MS vs. PS, 6% vs. 6%, respectively, P>0.99).
Conclusions: Prolonged PBD with NAC did not adversely affect surgical outcomes. MS placement provides a long patency period and is currently useful in PBD for PDAC patients undergoing PD after NAC, which requires a prolonged preoperative period. However, MS placement also has adverse events, and further studies are needed.
背景:近年来,新辅助化疗(NAC)越来越多地用于胰腺导管腺癌(PDAC)患者。这迫使术前胆道引流(PBD)在计划行胰十二指肠切除术(PD)的PDAC患者中的实践发生了变化。NAC时代发生了什么变化?什么是合适的PBD方法?为了解决这个问题,本研究回顾性回顾了NAC和前期手术(US)患者的手术结果和PBD的细节。方法:该研究纳入了2013年至2021年从US到NAC过渡期间连续接受PD治疗的PDAC患者,结果具有可比性。比较NAC组(40例)和US组(59例)患者的临床因素,如患者背景、术前检查、手术方式和术后并发症,并比较NAC组和US组(27例NAC组,33例US组)接受PBD的PBD的细节,如PBD程序和不良事件。在组间比较检验中,主要采用Fisher’s exact检验和Mann-Whitney U检验。此外,对60名接受PBD的患者进行了128种PBD手术的结果和通畅期的检查。采用Kaplan-Meier法进行log-rank检验,比较PBD程序的通畅期。结果:NAC组和US组患者背景无差异。与US组相比,NAC组术前白蛋白(ALB)水平较高,出血量较少,但术后并发症无差异(NAC组与US组分别为35% vs 46%, P=0.29)。关于PBD, NAC组有更多的初始金属支架(MS)置入(NAC vs. US,分别为52% vs. 15%, P=0.009),较少的PBD相关不良事件(NAC vs. US,分别为33% vs. 61%, P=0.04)。在引流方法的结果比较中,MS置入的通畅时间明显长于塑料支架(PS)置入的通畅时间(中位通畅天数,MS vs. PS, 68 vs. 15, pv)。PS, 6% vs. 6%, P>0.99)。结论:NAC患者长期PBD对手术结果没有不良影响。MS放置提供了较长的通畅期,目前在NAC后接受PD的PDAC患者的PBD中很有用,这需要较长的术前时间。然而,MS放置也有不良事件,需要进一步的研究。
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


