Casper Binding, Mariam Elmegaard, Deewa Zahir Anjum, Nicholas Carlson, Morten Schou, Anders Nissen Bonde
{"title":"Urinary albumin-to-creatinine ratio in patients with hypertension and risk of major cardiovascular events.","authors":"Casper Binding, Mariam Elmegaard, Deewa Zahir Anjum, Nicholas Carlson, Morten Schou, Anders Nissen Bonde","doi":"10.1136/openhrt-2025-003270","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction/aims: </strong>Evaluation of urinary albumin-to-creatinine ratio (uACR) is a key component in the management of hypertension, yet there is a lack of data on the association between uACR and major cardiovascular events (MACEs) in large hypertensive cohorts, and it is also unknown how often uACR is measured among these patients.We aimed to evaluate the usage of uACR in a nationwide population of patients with hypertension. Furthermore, we sought to assess the risk of cardiorenal events according to uACR, among patients with hypertension.</p><p><strong>Methods: </strong>We used Danish nationwide registries to identify patients who initiated antihypertensive treatment. The patients were grouped at treatment initiation according to uACR: normoalbuminuria, microalbuminuria, macroalbuminuria and no uACR measurement, and followed for 2 years, to evaluate the risk of a MACE, hospitalisation for heart failure (HF), 40% decline in estimated glomerular filtration rate (eGFR) and end-stage kidney disease (ESKD) according to uACR.</p><p><strong>Results: </strong>We included 144 644 patients, of whom 116 039 (80%) did not have their uACR evaluated at treatment initiation. Patients with macroalbuminuria comprised the greatest 2 year absolute risk of MACE (5.3%, 95% CI: 4.0% to 6.6%) and had a greater risk of MACE (HR: 2.02, 95% CI: 1.54 to 2.66), HF (HR: 1.99, 95% CI: 1.35 to 2.95), 40% decline in eGFR (HR: 4.81, 95% CI: 3.78 to 6.10) and ESKD (HR: 4.52, 95% CI: 3.00 to 6.82) compared with patients with normoalbuminuria. Increased risk of MACE, HF and 40% decline in eGFR among patients with macroalbuminuria was persistent across subgroups of eGFR 120-30 mL/min/1.73 m².</p><p><strong>Conclusions: </strong>In this real-world cohort, uACR was not regularly measured among patients initiating antihypertensive treatment. Nonetheless, the 2-year risks of cardiorenal events were considerably higher among patients with albuminuria compared with patients without.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097050/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003270","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction/aims: Evaluation of urinary albumin-to-creatinine ratio (uACR) is a key component in the management of hypertension, yet there is a lack of data on the association between uACR and major cardiovascular events (MACEs) in large hypertensive cohorts, and it is also unknown how often uACR is measured among these patients.We aimed to evaluate the usage of uACR in a nationwide population of patients with hypertension. Furthermore, we sought to assess the risk of cardiorenal events according to uACR, among patients with hypertension.
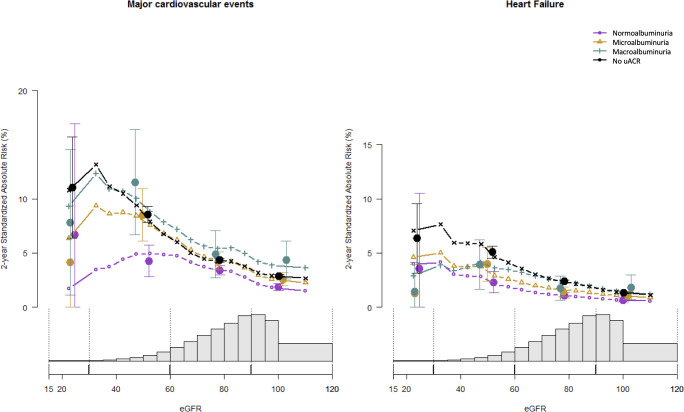
Methods: We used Danish nationwide registries to identify patients who initiated antihypertensive treatment. The patients were grouped at treatment initiation according to uACR: normoalbuminuria, microalbuminuria, macroalbuminuria and no uACR measurement, and followed for 2 years, to evaluate the risk of a MACE, hospitalisation for heart failure (HF), 40% decline in estimated glomerular filtration rate (eGFR) and end-stage kidney disease (ESKD) according to uACR.
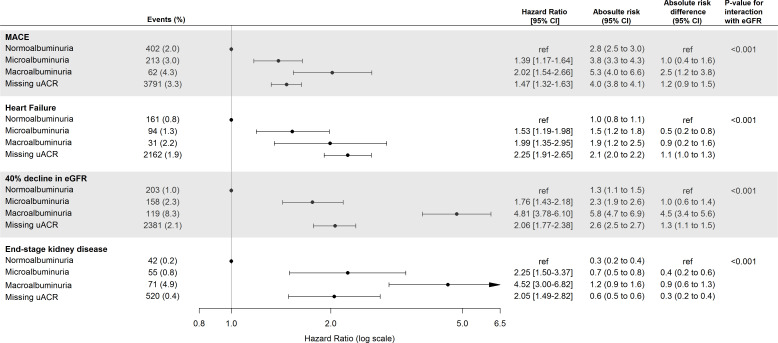
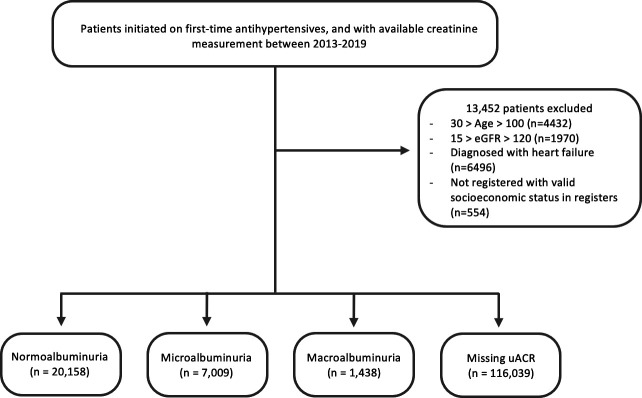
Results: We included 144 644 patients, of whom 116 039 (80%) did not have their uACR evaluated at treatment initiation. Patients with macroalbuminuria comprised the greatest 2 year absolute risk of MACE (5.3%, 95% CI: 4.0% to 6.6%) and had a greater risk of MACE (HR: 2.02, 95% CI: 1.54 to 2.66), HF (HR: 1.99, 95% CI: 1.35 to 2.95), 40% decline in eGFR (HR: 4.81, 95% CI: 3.78 to 6.10) and ESKD (HR: 4.52, 95% CI: 3.00 to 6.82) compared with patients with normoalbuminuria. Increased risk of MACE, HF and 40% decline in eGFR among patients with macroalbuminuria was persistent across subgroups of eGFR 120-30 mL/min/1.73 m².
Conclusions: In this real-world cohort, uACR was not regularly measured among patients initiating antihypertensive treatment. Nonetheless, the 2-year risks of cardiorenal events were considerably higher among patients with albuminuria compared with patients without.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


