Performance of the GRACE and the ACTION risk model in the prediction of in-hospital mortality: external validation, model revision and updating in the Thai Percutaneous Coronary Intervention Registry.
{"title":"Performance of the GRACE and the ACTION risk model in the prediction of in-hospital mortality: external validation, model revision and updating in the Thai Percutaneous Coronary Intervention Registry.","authors":"Songsak Kiatchoosakun, Noppadol Chamnarnphol, Chaiyasith Wongwipaporn, Burabha Pussadhamma, Worawut Roongsangmanoon, Sukanya Siriyotha, Ammarin Thakkinstian, Nakarin Sansanayudh","doi":"10.1136/openhrt-2024-003027","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>External validation is crucial before implementing a risk score model in clinical practice. This study examined the performance of Global Registry of Acute Coronary Events (GRACE) and Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Registry-Get With The Guidelines (GWTG) (ACTION Registry-GWTG) Risk Score (AR-G RS) using the Thai Percutaneous Coronary Intervention Registry (TPCIR).</p><p><strong>Methods: </strong>Included in this study were 11 455 patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) between November 2015 and May 2018. GRACE and AR-G RS models were externally validated, revised and updated using discrimination (C-statistic score) and calibration (Hosmer-Lemeshow (HL) indexes). Clinical predictors were selected stepwise from the multivariate analysis to evaluate the performance of each risk score in the revised and updated model.</p><p><strong>Results: </strong>In-hospital mortality was 4.4%. GRACE and AR-G RS demonstrated good discrimination for in-hospital mortality (C-statistics 0.8957 and 0.8823, respectively) with optimal calibration (HL, p=0.036 and 0.006, respectively) and penalty rates of 0.005 and 0.006, respectively. The updated model significantly improved the discrimination performance compared with the original GRACE and AR-G RS models, with a C-statistic of 0.9118 and a penalty of 0.006.</p><p><strong>Conclusion: </strong>GRACE and AR-G RS maintained a good performance in TPCIR. Based on routine PCI practice, we demonstrated that the updated model could improve the accuracy of GRACE and AR-G RS in predicting in-hospital mortality among patients with ACS who underwent PCI.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097003/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2024-003027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: External validation is crucial before implementing a risk score model in clinical practice. This study examined the performance of Global Registry of Acute Coronary Events (GRACE) and Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Registry-Get With The Guidelines (GWTG) (ACTION Registry-GWTG) Risk Score (AR-G RS) using the Thai Percutaneous Coronary Intervention Registry (TPCIR).
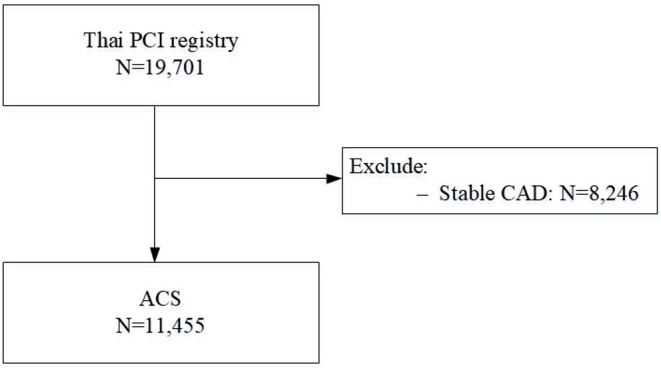
Methods: Included in this study were 11 455 patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) between November 2015 and May 2018. GRACE and AR-G RS models were externally validated, revised and updated using discrimination (C-statistic score) and calibration (Hosmer-Lemeshow (HL) indexes). Clinical predictors were selected stepwise from the multivariate analysis to evaluate the performance of each risk score in the revised and updated model.
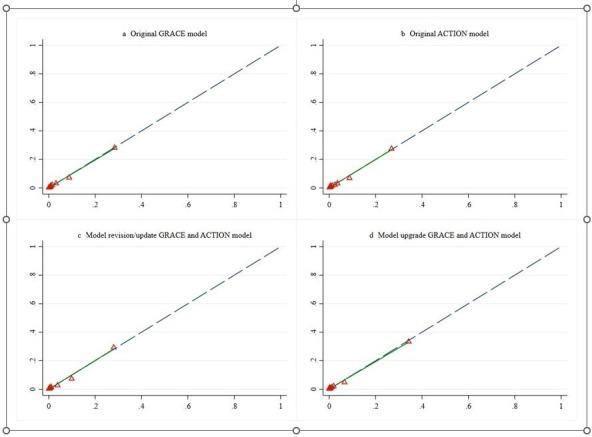
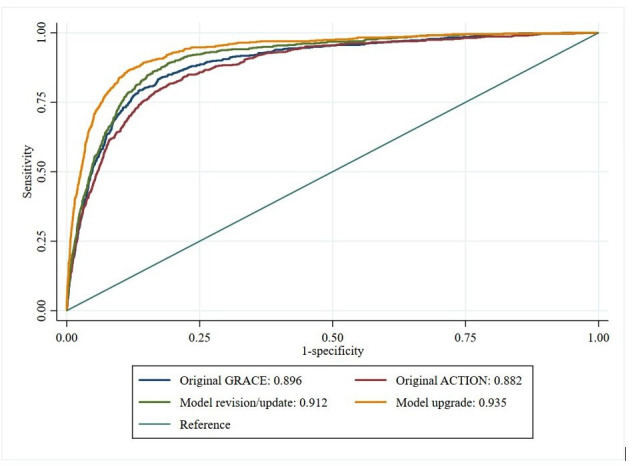
Results: In-hospital mortality was 4.4%. GRACE and AR-G RS demonstrated good discrimination for in-hospital mortality (C-statistics 0.8957 and 0.8823, respectively) with optimal calibration (HL, p=0.036 and 0.006, respectively) and penalty rates of 0.005 and 0.006, respectively. The updated model significantly improved the discrimination performance compared with the original GRACE and AR-G RS models, with a C-statistic of 0.9118 and a penalty of 0.006.
Conclusion: GRACE and AR-G RS maintained a good performance in TPCIR. Based on routine PCI practice, we demonstrated that the updated model could improve the accuracy of GRACE and AR-G RS in predicting in-hospital mortality among patients with ACS who underwent PCI.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


