Henock G Yebyo, Huldrych F Guenthard, Eva A Rehfuess, Nicola Serra, Sarah R Haile, Oliver Senn, Gregory M Lucas, Oliver Langselius, Jennifer E Thorne, Vincent C Marconi, Sally B Coburn, Raynell Lang, Jonathan A Colasanti, Michael J Silverberg, Sonia Napravnik, Mona Loutfy, Maile Karris, Timothy R Sterling, Greer A Burkholder, Keri N Althoff, Milo A Puhan
{"title":"Statins for primary prevention of cardiovascular events in people with HIV: target trial and modelling study.","authors":"Henock G Yebyo, Huldrych F Guenthard, Eva A Rehfuess, Nicola Serra, Sarah R Haile, Oliver Senn, Gregory M Lucas, Oliver Langselius, Jennifer E Thorne, Vincent C Marconi, Sally B Coburn, Raynell Lang, Jonathan A Colasanti, Michael J Silverberg, Sonia Napravnik, Mona Loutfy, Maile Karris, Timothy R Sterling, Greer A Burkholder, Keri N Althoff, Milo A Puhan","doi":"10.1136/bmjmed-2024-001132","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the effectiveness and benefit-harm balance of various statins for the primary prevention of cardiovascular disease in people with HIV.</p><p><strong>Design: </strong>Target trial and modelling study.</p><p><strong>Setting: </strong>North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD), 1995 to 2019. NA-ACCORD integrates individual level data from >20 HIV cohorts across the US and Canada from people with HIV who have successfully linked into care.</p><p><strong>Participants: </strong>157 699 people with HIV enrolled in one of the cohorts of NA-ACCORD. 54 165 eligible individuals, aged 40-75 years, were enrolled in the target trial.</p><p><strong>Main outcome measures: </strong>The primary outcomes for the target trial were the 10 year effects of statins on cardiovascular disease events (fatal and non-fatal myocardial infarction, hospital admission for unstable angina, coronary or arterial revascularisation, fatal and non-fatal stroke, or transient ischaemic attack) and harm outcomes (type 2 diabetes, mild cognitive impairment, rhabdomyolysis, and myopathy). The secondary outcome was the 10 year risk threshold where the reduction in cardiovascular disease outweighed the increased risk of harm outcomes, showing an overall net benefit of statins.</p><p><strong>Results: </strong>Participants who first started receiving treatment with statins (statin initiators) had a 21% reduction in cardiovascular disease events (hazard ratio 0.79, 95% confidence interval (CI) 0.72 to 0.87) and a 26% reduction in the combined risk of stroke and myocardial infarction (0.74, 0.56 to 0.98), but a 12% increase in the risk of type 2 diabetes (1.12, 1.01 to 1.25) compared with participants who developed the indication but did not take statins (non-initiators). The effects on cognitive impairment (hazard ratio 1.13, 95% CI 0.82 to 1.56), myopathy (1.10, 0.76 to 1.61), and rhabdomyolysis (1.09, 0.68 to 1.75) were not statistically significant. On average, the benefit of statins exceeded harms for individuals with a 10 year baseline risk of cardiovascular disease of ≥13.8%. Subgroup specific thresholds included men (14.2%), women (11.1%), ages 40-64 years (13.8%) versus 65-75 years (15.1%), and CD4 count >200 cells/mm³ (13.6%) versus <200 cells/mm³ (15.3%). Varying weights for cardiovascular disease yielded thresholds ranging from 11.6% to 54.0%, whereas weights for harm outcomes resulted in thresholds ranging from 5.0% to >30.0%.</p><p><strong>Conclusions: </strong>In this study, statins benefitted individuals with HIV with a moderate or high risk of cardiovascular disease, but the threshold for net benefit varied by patient subgroup and preference, implying the need to customise statin treatment to individual risks, preferences, and treatment goals. Given the limitations of observational data, further controlled studies are needed to evaluate the efficacy and safety of statins in people with HIV receiving modern antiretroviral therapy.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"4 1","pages":"e001132"},"PeriodicalIF":10.0000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12090529/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2024-001132","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate the effectiveness and benefit-harm balance of various statins for the primary prevention of cardiovascular disease in people with HIV.
Design: Target trial and modelling study.
Setting: North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD), 1995 to 2019. NA-ACCORD integrates individual level data from >20 HIV cohorts across the US and Canada from people with HIV who have successfully linked into care.
Participants: 157 699 people with HIV enrolled in one of the cohorts of NA-ACCORD. 54 165 eligible individuals, aged 40-75 years, were enrolled in the target trial.
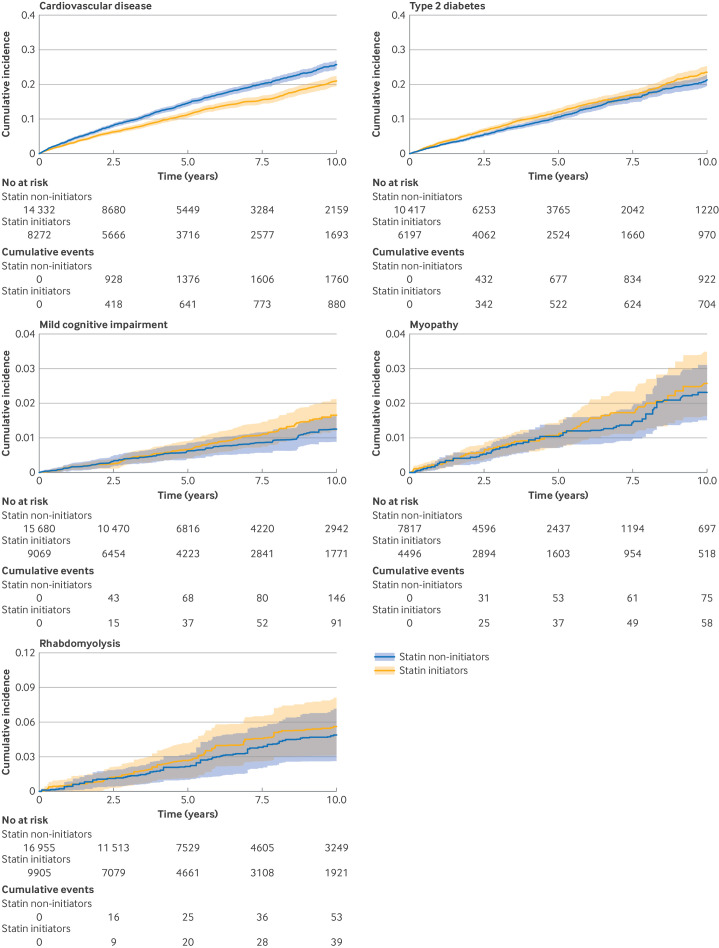
Main outcome measures: The primary outcomes for the target trial were the 10 year effects of statins on cardiovascular disease events (fatal and non-fatal myocardial infarction, hospital admission for unstable angina, coronary or arterial revascularisation, fatal and non-fatal stroke, or transient ischaemic attack) and harm outcomes (type 2 diabetes, mild cognitive impairment, rhabdomyolysis, and myopathy). The secondary outcome was the 10 year risk threshold where the reduction in cardiovascular disease outweighed the increased risk of harm outcomes, showing an overall net benefit of statins.
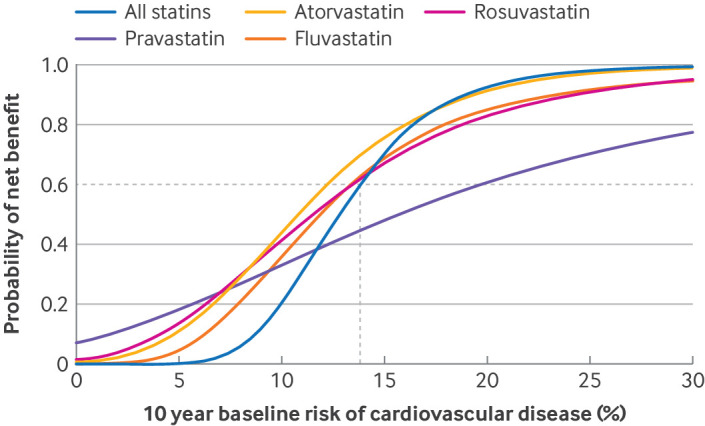
Results: Participants who first started receiving treatment with statins (statin initiators) had a 21% reduction in cardiovascular disease events (hazard ratio 0.79, 95% confidence interval (CI) 0.72 to 0.87) and a 26% reduction in the combined risk of stroke and myocardial infarction (0.74, 0.56 to 0.98), but a 12% increase in the risk of type 2 diabetes (1.12, 1.01 to 1.25) compared with participants who developed the indication but did not take statins (non-initiators). The effects on cognitive impairment (hazard ratio 1.13, 95% CI 0.82 to 1.56), myopathy (1.10, 0.76 to 1.61), and rhabdomyolysis (1.09, 0.68 to 1.75) were not statistically significant. On average, the benefit of statins exceeded harms for individuals with a 10 year baseline risk of cardiovascular disease of ≥13.8%. Subgroup specific thresholds included men (14.2%), women (11.1%), ages 40-64 years (13.8%) versus 65-75 years (15.1%), and CD4 count >200 cells/mm³ (13.6%) versus <200 cells/mm³ (15.3%). Varying weights for cardiovascular disease yielded thresholds ranging from 11.6% to 54.0%, whereas weights for harm outcomes resulted in thresholds ranging from 5.0% to >30.0%.
Conclusions: In this study, statins benefitted individuals with HIV with a moderate or high risk of cardiovascular disease, but the threshold for net benefit varied by patient subgroup and preference, implying the need to customise statin treatment to individual risks, preferences, and treatment goals. Given the limitations of observational data, further controlled studies are needed to evaluate the efficacy and safety of statins in people with HIV receiving modern antiretroviral therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


